What Works for Scars: The Science of Smooth Skin
From silicone gels to fractional lasers, this guide ranks every major scar treatment by clinical evidence — and tells you which ones to skip.
Proven Scar Treatments
What works for scars depends on the scar type, age, and location — but clinical evidence points to several consistently effective approaches:
| Treatment | Best For | Evidence Strength |
|---|---|---|
| Silicone gel/sheets | Raised, hypertrophic, post-surgical scars | Strong (meta-analyses) |
| Corticosteroid injections | Keloids, hypertrophic scars | Strong |
| Microneedling + PRP/PRF | Atrophic/acne scars | Moderate-strong |
| Pulsed dye laser (PDL) | Red, raised, vascular scars | Moderate |
| Moist wound care (petroleum jelly) | Fresh wounds/prevention | Strong |
| Adapalene 0.3% | Atrophic acne scars | Preliminary |
| Dermabrasion/chemical peels | Surface texture irregularities | Moderate |
| Scar massage | Post-surgical, mature scars | Moderate |
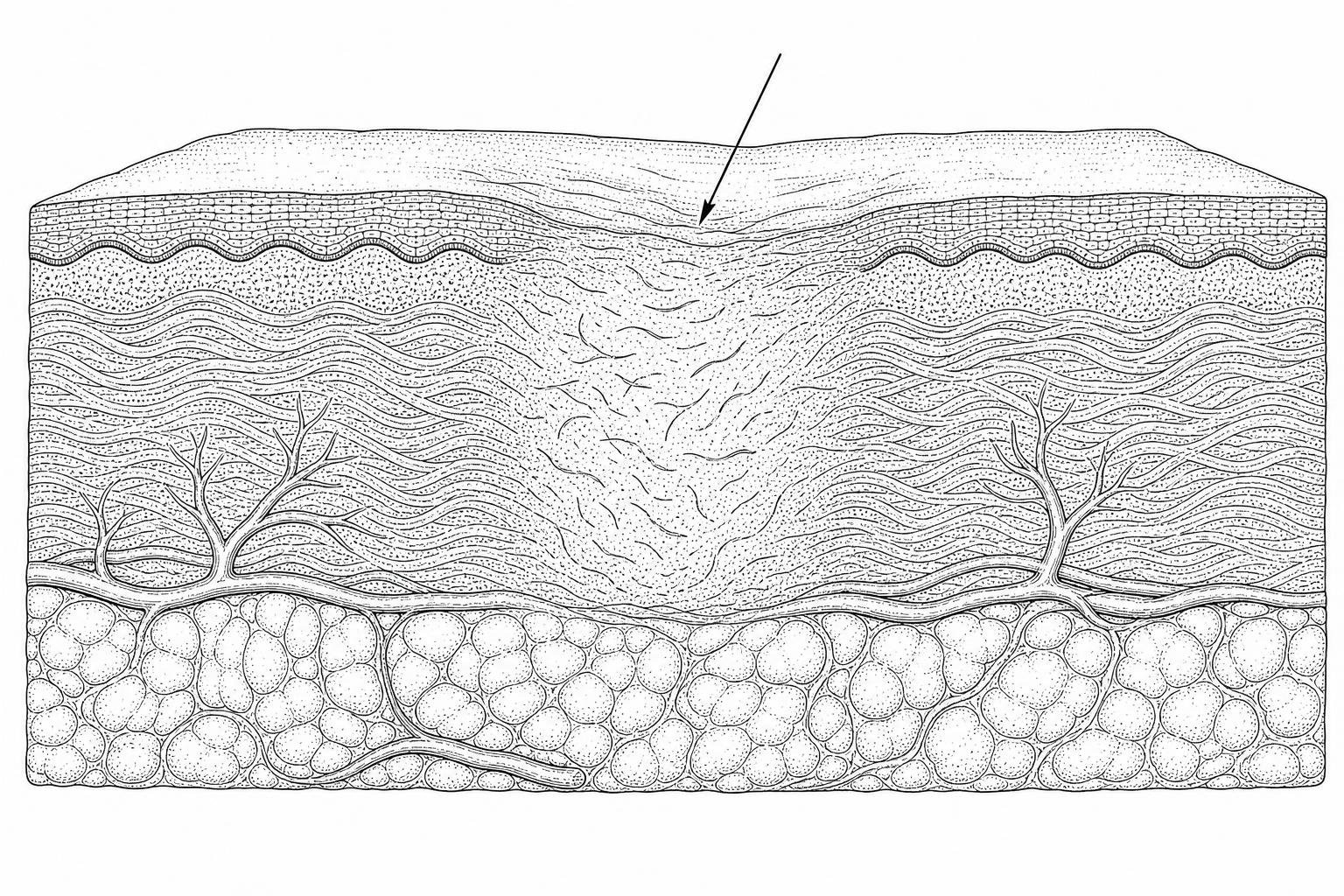
Scars are a natural outcome of how skin heals. When the dermis — the deeper layer of skin — is damaged, the body repairs it using collagen fibers. This repair process is fast and functional, but it does not restore the original skin architecture perfectly. The result is scar tissue: structurally different, visually distinct, and in some cases functionally limiting.
Nearly everyone carries at least one scar from an accident, surgery, acne, or illness. Yet despite how common them are, no single treatment eliminates a scar completely. What treatments can do — and do well, in many cases — is significantly reduce a scar's visibility, texture, color, and discomfort.
The challenge is that scars are not all the same. A raised requires a fundamentally different approach than a pitted acne scar. A fresh post-surgical scar responds to different interventions than one that is two years old. Matching the right treatment to the right scar type is the most important factor in getting results.
This guide reviews what the current clinical evidence actually shows — across topical therapies, injections, laser treatments, regenerative procedures, and prevention strategies — so that treatment decisions can be grounded in science rather than marketing.
How Scars Form and What Types Exist

Understanding what works for scars requires a look at the biological events that occur beneath the skin's surface. Scarring is an evolutionary compromise; the body prioritizes rapid wound closure to prevent infection over the slow restoration of perfect skin.
How Your Skin Repairs Itself
When an injury penetrates the dermis, the healing process unfolds in three distinct but overlapping phases:
- The Inflammatory Phase: Immediately after injury, blood clots form and white blood cells migrate to the site to clear debris and bacteria.
- The Proliferative Phase: Fibroblasts—the primary functional cells of the dermis—begin synthesizing new extracellular matrix (ECM) and collagen. In a scar, this collagen is deposited in dense, parallel bundles rather than the basket-weave pattern found in healthy skin.
- The Maturation Phase: Also known as remodeling, this phase can last up to two years. The body attempts to break down excess collagen and reorganize the fibers. This is why many scars naturally fade and soften over 12 to 18 months.
More info about post-surgery scar care can help navigate this timeline more effectively.
Identifying Scar Phenotypes
Effective treatment is impossible without accurate classification. Clinical consensus categorizes scars into several distinct phenotypes:
- Flat Scars: Initially red or pink, these eventually become pale and slightly sunken or raised.
- Hypertrophic Scars: Raised and red, these stay within the boundaries of the original wound. They often form in areas of high skin tension, such as the back or joints.
- Keloid Scars: These are aggressive overgrowths of scar tissue that extend beyond the original injury site. They can be painful or itchy and are more common in individuals with darker skin tones or red hair.
- Atrophic Scars: Sunken or pitted, these result from a loss of underlying fat or muscle tissue. Acne and chickenpox are the most common causes.
- Contracture Scars: Often resulting from burns, these cause the skin to tighten, potentially restricting movement if they occur over joints.
Table: Keloid vs. Hypertrophic Characteristics
| Feature | Hypertrophic Scar | Keloid Scar |
|---|---|---|
| Growth Boundary | Remains within wound edges | Extends beyond wound edges |
| Natural Regression | May flatten over time | Rarely regresses spontaneously |
| Common Sites | Joints, neck, abdomen | Earlobes, chest, shoulders |
| Onset | Shortly after injury | Can appear months or years later |
For a deeper dive into causes, see Scars: Treatment and Cause.
First-Line Scar Therapies: What the Evidence Shows

When determining what works for scars in a clinical setting, dermatologists typically start with non-invasive topical treatments or localized injections.
Silicone and Hydration in Scar Management
Since its introduction in the early 1980s, silicone has remained the gold-standard non-invasive therapy. It is available in two primary forms: gel sheets and topical gels.
Research published in the Journal of Drugs in Dermatology suggests that silicone's efficacy stems from its ability to provide occlusion and hydration. By mimicking the skin's barrier, silicone reduces transepidermal water loss (TEWL). This hydration signals to the fibroblasts to decrease collagen production, which helps flatten and soften the tissue.
- Usage Protocol: For optimal results, silicone sheets should be worn for at least 12 hours a day (ideally 24 hours) for several months.
- Efficacy: Clinical data indicates a mean scar thickness reduction of 37% (with a range of 20-54%) after six months of consistent use.
More info about silicone for hypertrophic scars provides specific application tips for raised tissue. Knowing when to start scar treatment is also critical; silicone therapy usually begins once the wound has fully re-epithelialized (closed).
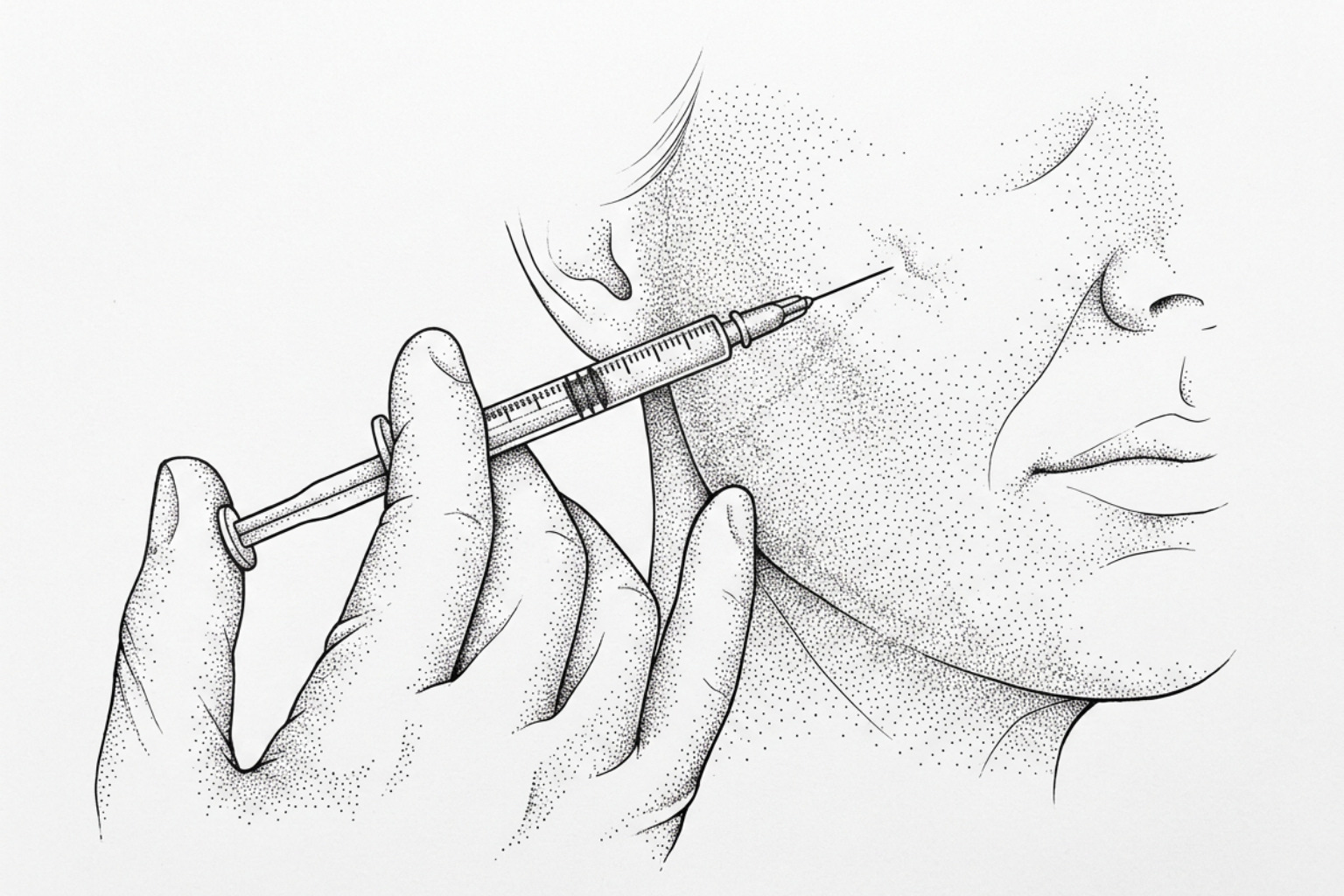
Corticosteroid Injections for Raised Tissue
For stubborn hypertrophic scars and keloids that do not respond to topicals, intralesional corticosteroid injections (typically triamcinolone acetonide) are highly effective.
These injections work by suppressing inflammation and inhibiting fibroblast proliferation. According to clinical statistics, corticosteroid injections can reduce the size of a raised scar by 50% or more. Treatments are usually administered in a series, spaced 4 to 6 weeks apart.
While effective, potential side effects include skin thinning (atrophy) or changes in pigmentation at the injection site. For more on managing these types of scars, see More info about non-invasive keloid management.
Lasers vs. surface treatments
Laser technology has transformed the field of scar revision, offering precise ways to target redness and texture.
Lasers for redness and texture
The choice of laser depends on the scar’s color and thickness:
- Pulsed Dye Laser (PDL): Operating at a 595 nm wavelength (such as the V-beam), this laser targets the blood vessels within the scar. It is the primary choice for reducing the redness (erythema) of fresh or hypertrophic scars.
- Ablative Fractional CO2 Lasers: These create microscopic columns of injury in the skin, "drilling" through the scar tissue to stimulate the production of new, organized collagen. A single session can improve scar softness and irregularities by up to 30%.
- Non-Ablative Lasers: These stimulate collagen remodeling without damaging the skin's surface, leading to shorter recovery times but often requiring more sessions.
For detailed guidance on surgical scars, see More info about laser treatment for surgical scars and More info about red scar fading.
Surface Resurfacing: Dermabrasion and Chemical Peels
Before the advent of lasers, dermabrasion and chemical peels were the primary methods for smoothing scars.
- Dermabrasion: A surgical procedure where the top layers of skin are "sanded" down. It is effective for treating surface irregularities but carries a higher risk of pigmentation changes, especially in darker skin tones.
- Chemical Peels: Using acids like trichloroacetic acid (TCA) or glycolic acid, these peels remove the stratum corneum and stimulate epidermal turnover. They are most commonly used for mild acne scarring.
More info about chemical peel scar revision explores how these acids are used to normalize skin texture.
Specialized Protocols for Atrophic and Acne Scars
Atrophic scars, characterized by "pits" or indentations, require treatments that "bulk up" the tissue from beneath.
Microneedling and Regenerative Injections for Pitted Scars
Microneedling, or collagen induction therapy, involves using fine needles to create controlled micro-injuries. When combined with Platelet-Rich Plasma (PRP) or Platelet-Rich Fibrin (PRF), the results are significantly enhanced.
- The Evidence: A comparative study found that microneedling combined with PRP/PRF resulted in a 70.43% mean improvement in atrophic scars. This is significantly higher than PRP alone (48.82%) or microneedling alone (39.71%).
- The Protocol: Clinical guidelines suggest a needle depth of 1.5mm for most atrophic scars, with sessions spaced one month apart.
For more information, see More info about microneedling for atrophic scars and the More info about non-invasive acne scar guides.
Treatments for pitted scars
Topical retinoids are not just for active acne; they also play a role in scar remodeling. Adapalene gel 0.3% has shown promise in treating atrophic acne scars. In a 24-week study, 55.6% of patients demonstrated a 1- or 2-grade improvement on a global scarring scale.
Retinoids work by increasing cell turnover and stimulating collagen production over time. More info about pimple scar removal details how to integrate these into a long-term routine.
Evidence-Based Prevention and Home Care Strategies
The best way to treat a scar is to minimize its formation during the initial healing phase. Modern wound care has debunked many "old school" methods.
Immediate Post-Injury Protocols
The goal of early wound care is to reduce inflammation and tension.
- Keep it Moist: Contrary to the advice to "let it air out," wounds heal faster and with less scarring when kept moist. Applying petroleum jelly (Vaseline) and covering the area with a clean bandage is the most effective way to prevent hard scabs. Scabs act as biological "speed bumps" that interfere with smooth skin regeneration.
- Sun Protection: UV exposure is the enemy of a healing scar. It can cause permanent hyperpigmentation (darkening) and break down the fragile new collagen. Using a broad-spectrum SPF 30+ sunscreen or keeping the area covered for at least one year is essential.
- Tension Reduction: If a wound is in a high-movement area, limiting activity can prevent the scar from stretching and becoming a "fine-line" or hypertrophic scar.
More info about applying cream after stitches provides a timeline for starting these interventions.
Long-Term Maintenance and Maturation
Scars are dynamic. They continue to remodel for up to two years. During the first year, mechanical remodeling through massage can be beneficial.
- Scar Massage: Once the wound is fully closed and any stitches are removed, massaging the scar for 1 to 2 minutes, 1 to 3 times per day, can help break up dense collagen bundles and soften the tissue.
- The Timeline: Most scars will reach their "mature" state (becoming paler and softer) by the 18-month mark.
For techniques, see More info about scar tissue massage therapy.
Frequently Asked Questions about Scar Healing
Are natural remedies like Vitamin E or honey effective?
The evidence for common home remedies is mixed at best.
- Vitamin E: Despite its popularity, multiple studies show that topical Vitamin E does not consistently improve scar appearance. In fact, up to 33% of users develop contact dermatitis (a skin rash) from it. More info about Vitamin E research highlights these risks.
- Honey: Medical-grade Manuka honey has potent anti-inflammatory and antibacterial properties that are excellent for wound healing. However, once a scar has already formed, there is no scientific evidence that honey can reduce its size or texture.
- Aloe Vera: Some evidence suggests aloe vera can aid in the early wound-healing phase, but it is not considered a primary treatment for mature scars.
How long does it take for a scar to fade naturally?
The natural fading process is slow. Most scars go through a "red and angry" phase for the first 3 to 6 months. After this, they typically begin to fade to a white or silvery color. Complete maturation usually takes 12 to 18 months, though larger or more severe injuries can take up to two years. If a scar has not improved after two years, it is unlikely to change further without medical intervention.
When should a specialist be consulted for scar revision?
While many scars are purely cosmetic concerns, some require professional intervention. You should consult a dermatologist or plastic surgeon if:
- The scar is painful, persistently itchy, or tender.
- The scar is growing rapidly (suggesting a keloid).
- The scar restricts your movement or "pulls" on your skin (contracture).
- The scar is causing significant psychological distress or impacting your quality of life.
More info about surgical scar revision covers the options available for these more complex cases.
Building Your Evidence-Based Scar Care Plan
Determining what works for scars requires moving past marketing claims and looking at clinical data. For raised scars, the combination of silicone therapy and corticosteroid injections remains the gold standard. For atrophic or acne scars, regenerative techniques like microneedling with PRP offer the highest rates of improvement.
The most effective scar treatment is prevention through diligent wound care and sun protection. Because every skin type and injury is unique, an individualized approach is necessary for the best clinical outcomes.
Start your professional scar assessment to determine which evidence-based path is right for your skin.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/
- Gold, M. H., et al. (2014). Updated international clinical recommendations on scar management: Part 2. Dermatologic Surgery, 40(8), 825–831. https://pubmed.ncbi.nlm.nih.gov/25068544/
- Monstrey, S., et al. (2014). Updated scar management practical guidelines. Journal of Plastic, Reconstructive & Aesthetic Surgery, 67(8), 1017–1025. https://pubmed.ncbi.nlm.nih.gov/24888226/
- Khansa, I., Harrison, B., & Janis, J. E. (2016). Evidence-Based Scar Management. Plastic and Reconstructive Surgery, 138(3 Suppl), 165S–178S. https://pubmed.ncbi.nlm.nih.gov/27556757/
- Gurtner, G. C., et al. (2008). Wound repair and regeneration. Nature, 453(7193), 314–321. https://pubmed.ncbi.nlm.nih.gov/18480812/