The Ultimate Guide to Hypertrophic Scar Flattening and Microneedling
A clinical review of microneedling for hypertrophic scar flattening — covering needle-depth protocols, Vancouver Scar Scale outcomes, radiofrequency adjuncts, and safety across all skin tones.
How Microneedling Flattens Raised Scars
Microneedling for hypertrophic scars is a clinically studied approach to flattening raised, thickened scar tissue by triggering the skin's own repair mechanisms. Here is what research currently shows:
| Question | Short Answer |
|---|---|
| Does microneedling flatten hypertrophic scars? | Evidence suggests yes — significant improvement documented across multiple clinical studies |
| How many sessions are needed? | Typically 3–6 sessions, spaced 4–6 weeks apart |
| How much improvement can be expected? | One prospective study recorded Vancouver Scar Scale scores dropping from 8.8 to 4.1 after sequential treatment |
| Is it safe for darker skin tones? | Evidence indicates radiofrequency microneedling carries lower pigmentation risk than laser alternatives |
| What works best alongside microneedling? | Triamcinolone delivery, PRP, and fractional radiofrequency are the most studied adjuncts |
Raised, firm, red scars affect an estimated 15% of people following surgical incisions — and over 70% of burn survivors, according to published clinical literature. For an overview of burn-specific options, see this guide to burn scar treatments. For many, these marks are not simply cosmetic. They can restrict joint movement, cause persistent itching or pain, and significantly affect confidence and quality of life.
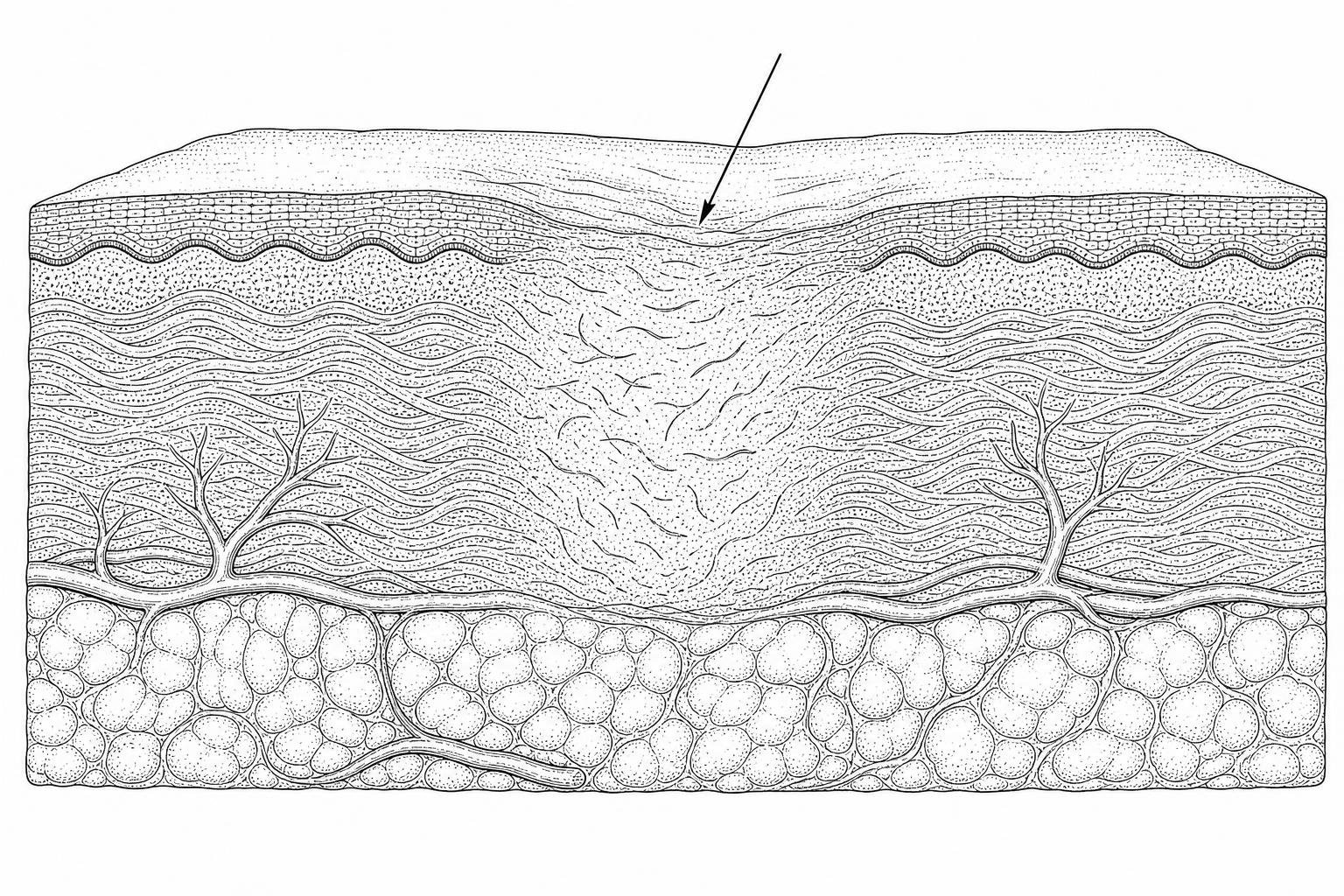
Hypertrophic scars form when the wound-healing process goes into overdrive. Specialized cells called fibroblasts — which normally produce collagen to close a wound — become overactive. They deposit excessive amounts of disorganized collagen, particularly type III collagen, creating tissue that is thicker, stiffer, and more vascular than surrounding skin. Unlike keloids, hypertrophic scars remain within the original wound boundary.
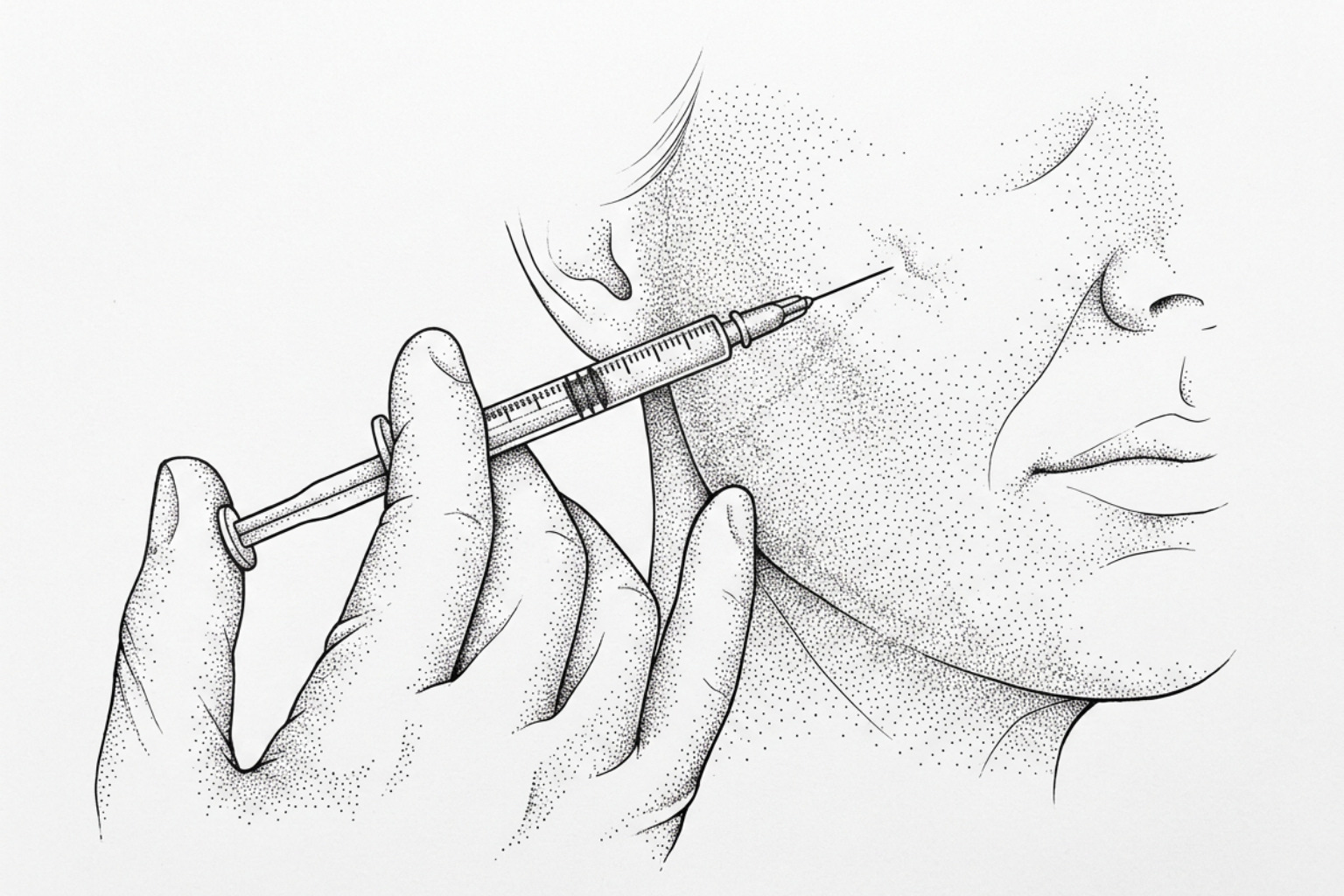
Microneedling, also described in clinical literature as minimally invasive percutaneous collagen induction, creates controlled micro-injuries in the dermis — the deeper layer of skin beneath the surface. This process disrupts the dense, fibrous scar architecture and stimulates the production of more organized, mature type I collagen, gradually remodeling the scar from within.
As of April 2026, a growing body of peer-reviewed evidence — including a systematic review of 58 studies involving 1,845 patients — supports microneedling as a viable, well-tolerated intervention for hypertrophic scars, particularly when combined with targeted drug delivery or adjunct therapies.
This guide examines the underlying biology of raised scars, reviews what clinical research actually shows about microneedling outcomes, and outlines what realistic expectations look like for someone considering this treatment.
Why Hypertrophic Scars Form
To understand why microneedling for hypertrophic scars is effective, one must first look at why these scars form. Physiological wound healing is a highly regulated four-stage process: hemostasis, inflammation, proliferation, and remodeling. In hypertrophic scarring, this regulation fails during the proliferative and remodeling phases.
Research indicates that prolonged inflammation, often driven by myeloid cells and mast cells, sustains the activity of myofibroblasts. These cells are responsible for wound contraction and collagen deposition. When they remain active for too long, they produce an abundance of Type III collagen arranged in rigid, parallel bundles rather than the healthy "basket-weave" pattern found in normal skin.
Hypertrophic Scars vs. Keloids
While both are considered "raised scars," they differ in clinical behavior:
- Hypertrophic Scars: These remain within the boundaries of the original injury. They often show a degree of natural regression over several years and are frequently associated with mechanical tension or delayed wound healing (such as in burns).
- Keloids: These extend beyond the original wound margins, invading healthy tissue. They rarely regress and have a higher recurrence rate after surgical excision. Learn more about non-surgical keloid treatments.
Mechanical tension is a primary driver of hypertrophy. Areas of high skin tension, such as the chest, shoulders, and joints, are more prone to developing these thick, raised marks. Scientific research on raised scar management suggests that microneedles may help by providing "mechanical off-loading," essentially disrupting the tension that keeps fibroblasts in an overactive state.
For those managing these conditions, understanding the specific type of scar is essential for choosing the right intervention. You can find more info about hypertrophic scars to help distinguish between these common skin concerns.
How Microneedling Triggers Collagen Growth
The therapeutic effect of microneedling is rooted in "percutaneous collagen induction." When the needles penetrate the skin, they create thousands of microscopic channels. This mechanical trauma initiates a controlled wound-healing cascade without significantly damaging the epidermis (the outermost layer).
Key biological changes observed during this process include:
- Release of Growth Factors: The micro-injuries trigger the release of vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF-7), and epidermal growth factor (EGF).
- Modulation of TGF-β: Transforming growth factor-beta (TGF-β) plays a dual role in scarring. While TGF-β1 and TGF-β2 promote scar formation, TGF-β3 is associated with scarless healing. Microneedling is thought to help balance these expressions.
- Dermal Remodeling: The physical disruption of the rigid Type III collagen bundles allows the skin to replace them with Type I collagen, which is more flexible and organized.
This cellular "reset" is why many clinicians view microneedling for scar reduction as a foundational treatment for improving skin texture and pliability.
Needle Depth and Treatment Protocol
Unlike microneedling for fine lines, which may only require shallow depths, treating hypertrophic tissue requires reaching the deep dermis where the dense collagen resides.
- Needle Depth: Clinical protocols for raised scars typically utilize depths between 1.5mm and 3.0mm. However, a systematic review noted that 1mm needles are often the most accurate in terms of actual penetration, as 3mm needles may only reach 1.5–2.0mm in dense scar tissue.
- Clinical Endpoint: The goal is usually "uniform pinpoint bleeding," which indicates the needles have reached the vascularized dermis.
- Technique: Clinicians often perform 4 to 10 passes in multiple directions (vertical, horizontal, and diagonal) to ensure comprehensive disruption of the scar tissue.
While some individuals attempt to use at-home tools, professional devices are generally required for the depths necessary to impact raised scars. For a deeper look at the tools used, see this info about dermarollers for scars.
Microneedling as a Drug-Delivery System
One of the most significant advancements in scar management is using microneedling as a delivery system. Because hypertrophic scars are dense, traditional topical creams often fail to penetrate deeply enough to be effective.
- Triamcinolone Acetonide (TAC): This corticosteroid is a first-line treatment for flattening scars. By microneedling first, the TAC can be spread topically and "pushed" into the micro-channels, or injected intralesionally with greater ease. Scientific research on microneedling for post-burn scars shows that this combination significantly improves scar height and redness.
- Platelet-Rich Plasma (PRP): Using the patient's own growth factors can accelerate the remodeling process and reduce downtime.
- Radiofrequency (RF) Microneedling: This involves needles that emit heat energy at their tips. The heat further tightens and remodels collagen, making it particularly effective for stubborn, thick scars. For a deeper look at RF devices, see this guide to laser and energy-based scar treatments.

Measured Results and Scar Scale Scores
Clinical efficacy is often measured using the Vancouver Scar Scale (VSS), which grades scars based on four criteria: pigmentation, vascularity, pliability, and height.
A prospective study of 15 patients with post-burn hypertrophic scars demonstrated the following:
- VSS Score Improvement: Average scores dropped from 8.8 ± 0.44 at baseline to 4.1 ± 0.98 after treatment (p = 0.012).
- Joint Mobility: For scars located over joints, there was a significant and progressive improvement in the range of motion.
- Texture: Patients reported scars becoming softer and less "bound down" to underlying tissues. Complementary techniques such as scar tissue massage therapy can reinforce this softening between sessions.
Further evidence from a case report involving refractory scars (those that did not respond to previous laser or steroid treatments) showed that radiofrequency microneedling and corticosteroids could achieve flattening and redness reduction in as little as three weeks.
Real-World Outcomes for Post-Burn and Traumatic Scars
The timing of treatment appears to be a critical factor in success rates. Clinical data suggests that "acute" hypertrophic scars — those less than one year old — respond more robustly to microneedling than chronic, older scars. In one group, acute burn scars improved from a VSS of 9.3 to 3.5.
Patient satisfaction is notably high. In a review of 58 studies, 50% to 100% of patients reported being satisfied with their results, and 94% stated they would recommend the procedure to others. While microneedling may not "erase" a scar completely, the improvement in comfort and appearance is often life-changing for those with restrictive burn scars. For ongoing maintenance between sessions, many patients use hypertrophic scar silicone gel to keep the tissue hydrated and protected.
Safety Across Skin Tones
A major advantage of microneedling for hypertrophic scars over certain laser therapies is its safety profile for patients with Fitzpatrick Skin Types IV–VI (darker skin tones).
Laser treatments, particularly ablative fractional lasers, work by heating the water in the skin. This can cause collateral thermal damage to the epidermis, leading to a high risk of post-inflammatory hyperpigmentation (PIH) or hypopigmentation (loss of color) in darker skin.
Microneedling is "non-thermal" (unless RF is used) and leaves the epidermis mostly intact.
- RF Microneedling (RFMN): Use of insulated needles allows energy to be delivered only to the dermis, sparing the pigment-producing cells in the epidermis.
- PIH Risks: While lower than lasers, PIH can still occur. A 2020 systematic review found PIH in approximately 33% of studies, though it typically resolved spontaneously or with topical treatments.
- Tramtrack Scarring: A rare side effect where the pattern of the needles becomes visible, usually due to excessive pressure or improper technique.
Clinicians are advised to vary needle depth based on the anatomical area and to use disposable tips to minimize infection risk. For a comprehensive overview of safety, clinicians often refer to the latest microneedling updates.
Microneedling vs. Other Scar Treatments
When deciding on a treatment plan, it is helpful to compare microneedling with other standard-of-care options.
| Treatment | Mechanism | Primary Benefit | Main Risk/Drawback |
|---|---|---|---|
| Microneedling | Mechanical micro-injury | Low PIH risk; improves pliability | Requires multiple sessions |
| Fractional CO2 Laser | Thermal ablation | Significant flattening | High PIH risk in dark skin; long downtime |
| Intralesional Steroids | Anti-inflammatory | Fast flattening | Risk of skin atrophy (thinning) and telangiectasia |
| Silicone Sheets/Gels | Hydration/Occlusion | Non-invasive; easy to use | Slow results; must be worn 12-24 hrs/day |
While microneedling is highly effective, it is often used as part of a multi-modal approach. For a detailed comparison of laser modalities, see the laser scar reduction treatment guide. For instance, a patient might use hypertrophic scar reduction creams or silicone sheets daily while undergoing professional microneedling sessions every month.
Treatment FAQs and Aftercare
How Many Sessions Until You See Results
Most clinical studies utilize a protocol of 3 to 6 sessions. These are typically spaced 4 to 6 weeks apart to allow the skin's remodeling cycle to complete. While some initial softening may be felt after the first session, the most significant flattening usually occurs after the third or fourth treatment. Collagen remodeling can continue for up to 6 months after the final session.
Does Microneedling Work on Older Scars
Yes, though the response may be slower. Chronic scars are characterized by very dense, "mature" collagen. Microneedling can help "soften" this tissue, but it may require more sessions or a combination with radiofrequency to achieve the same results seen in newer scars. Early intervention (within the first year) is generally recommended for the best outcomes. More details can be found on best scar removal treatments for various scar ages.
What post-treatment care is essential for optimal healing?
Post-care is critical to prevent complications like infection or PIH.
- Sun Protection: The skin is highly sensitive to UV rays for several weeks post-treatment. Daily application of broad-spectrum SPF 30+ is mandatory.
- Bland Emollients: Use gentle, fragrance-free moisturizers to maintain the skin barrier.
- Avoid Irritants: Steer clear of retinoids, vitamin C serums, or exfoliating acids for at least 5–7 days.
- Hygiene: Do not touch the treated area with unwashed hands and avoid swimming or heavy sweating for 48 hours.
Proper aftercare ensures that the micro-channels heal without inflammation, which is especially important if you are also treating atrophic scars.
What This Means for Your Scar Journey
Hypertrophic scars can be a source of physical and emotional distress, but the evolution of microneedling for hypertrophic scars has provided a reliable, minimally invasive path to improvement. By disrupting disorganized collagen and facilitating the delivery of anti-fibrotic medications, microneedling addresses the root cause of the scar's thickness and rigidity.
While results are progressive rather than immediate, the high patient satisfaction rates and significant improvements in scar scales suggest that this therapy is a cornerstone of modern scar management. If you are ready to begin your journey toward smoother skin, you can start your scar assessment today to determine which approach is best for your specific scar type.
Works Cited:
- Microneedling in the Treatment of Post-burn Hypertrophic Scars. Aesthetic Plastic Surgery, 2024.
- Leveraging Microneedles for Raised Scar Management. Jin Z, Kim Y-S, Lim JY. Polymers, 2025.
- Combination Therapy Using Radiofrequency Microneedling and Corticosteroids for Hypertrophic Scars: A Case Report. Juhász M, Fackler N. J Clin Aesthet Dermatol, 2020.
- Microneedling for the Treatment of Scars: An Update for Clinicians. Clin Cosmet Investig Dermatol, 2020.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.