Piercing Problems: Non-Surgical Ways to Kiss Your Keloids Goodbye
Keloids can be treated without going under the knife. Explore evidence-based non-surgical options including silicone therapy, corticosteroid injections, and cryotherapy for piercing-related keloids.
Does Non-Surgical Keloid Treatment Work
Keloid treatment without surgery is a well-studied area of dermatology, and evidence supports several effective non-surgical options. Here is a quick clinical summary:
Evidence-based non-surgical options for keloids:
| Treatment | Evidence Level | Response Rate |
|---|---|---|
| Intralesional corticosteroid injections | Strong (first-line) | 50–100% |
| Silicone gel sheeting | Strong (gold standard noninvasive) | Up to 90% improvement |
| Cryotherapy | Moderate | 30–75% after 2 sessions |
| 5-Fluorouracil (5-FU) injections | Moderate | 45–96% |
| Pressure garment therapy | Moderate | Varies by compliance |
| Superficial radiation therapy (post-excision) | Strong | >90% cure rate |
| Laser therapy (pulsed-dye, CO2) | Moderate | Varies by keloid type |
Keloid scars have been documented as far back as ancient Egypt — and they continue to frustrate patients and clinicians alike. Nearly 18 million people are affected by them worldwide.
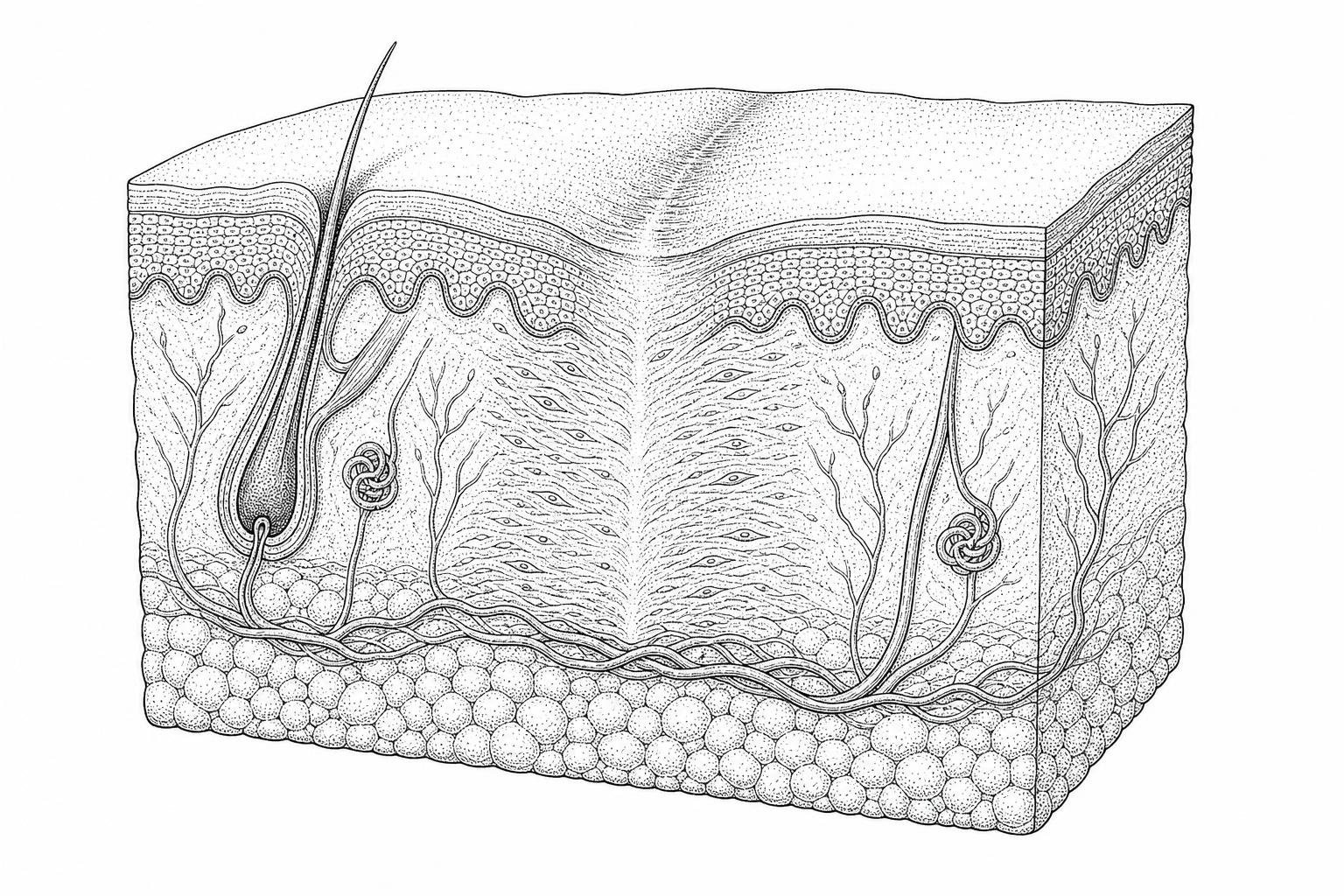
A keloid is not simply a large scar. It is a fibroproliferative disorder — meaning the body's wound-healing process becomes dysregulated, triggering excessive collagen deposition that grows beyond the boundaries of the original injury. This abnormal tissue expansion is driven by overactive fibroblasts (the cells responsible for producing collagen) and is strongly influenced by genetic predisposition. Keloids are significantly more common in individuals with darker skin tones, occurring in approximately 10% of the African-American population.
Unlike normal scars, keloids rarely resolve on their own. And while surgical removal might seem like the logical solution, surgery alone carries a recurrence rate of 45–100% — often resulting in a larger keloid than before.
That is why the clinical focus has shifted firmly toward non-surgical and multimodal approaches. The research reviewed here draws on peer-reviewed clinical guidelines, systematic reviews, and consensus recommendations from international dermatology panels to outline what the evidence actually supports.
What Makes Keloid Scars Different
To understand why keloid treatment without surgery is often the preferred starting point, one must look at the cellular level. When the skin is injured, the body initiates a complex repair sequence involving inflammation, proliferation, and maturation. In most people, this process concludes with a flat, pale scar. However, in keloid-prone individuals, the "off switch" for collagen production appears to be broken.
The primary driver of this dysfunction is the fibroblast. In a keloid, these cells produce between three and twenty times more collagen than in a normal healing wound. This excess collagen creates a dense, disorganized extracellular matrix that pushes outward, invading healthy surrounding skin.
Hypertrophic Scars vs. Keloids
It is clinically vital to distinguish keloids from hypertrophic scars, as their management differs. According to the Management of Keloids and Hypertrophic Scars | AAFP, hypertrophic scars are raised and red but remain strictly within the boundaries of the original wound. They often regress over time. Keloids, conversely, are "social climbers" of the scar world; they do not respect boundaries and rarely regress. They are frequently associated with pain, pruritus (itching), and significant psychological distress.
While keloids can affect anyone, genetic susceptibility is a major factor. They are 15 to 20 times more common in individuals with highly pigmented skin. Common "high-tension" sites for formation include the chest, shoulders, upper back, and earlobes—often following minor traumas like acne, piercings, or insect bites.
First-Line Non-Surgical Keloid Treatments
When a patient seeks keloid treatment without surgery, the most common medical recommendation is intralesional corticosteroid injection. This has been the clinical "gold standard" for decades.
Corticosteroid Injections: How They Work
The most frequently used agent is triamcinolone acetonide (TAC), typically administered in concentrations of 10 to 40 mg/mL. These injections work by:
- Inhibiting the inflammatory response.
- Reducing fibroblast proliferation.
- Decreasing collagen and glycosaminoglycan synthesis.
- Increasing the activity of collagenase, an enzyme that breaks down collagen.
Clinical data suggests a response rate of 50% to 100%, with many patients seeing significant flattening of the scar. However, it is rarely a "one and done" procedure. Most protocols require injections every 4 to 6 weeks for several months. While effective at reducing size and itchiness, recurrence rates remain a challenge, ranging from 9% to 50%.

For many patients, combining these injections with other modalities provides the best outcome. You can find more info about non-invasive removal strategies that utilize this multimodal approach to minimize the risk of the scar bouncing back.
How Silicone Therapy Manages Keloids
If injections are the heavy hitters of the medical world, silicone products are the essential support crew. Silicone gel sheeting has been used for over 30 years and is considered a first-line non-invasive treatment in international guidelines.
The Hydration Mechanism
Contrary to popular belief, silicone doesn't work through "pressure" alone. Instead, its primary mechanism is occlusion and hydration. By covering the scar, silicone reduces transepidermal water loss. This increased hydration signals the body to downregulate the production of collagen-producing cells. Research published in Management of keloid scars: noninvasive and invasive treatments - PMC indicates that silicone gel sheeting can lead to up to 90% improvement in the texture and color of keloid scars when used consistently.
Silicone Gels vs. Silicone Sheets
Patients often ask which format is superior. Clinical trials suggest they are equally effective, provided they are used for the recommended 12 to 24 hours per day for at least 3 to 6 months.
| Feature | Silicone Gel Sheets | Topical Silicone Gel |
|---|---|---|
| Application | Self-adhesive sheet | Spreadable gel |
| Best For | Large, flat areas (chest, back) | Visible areas (face, joints) |
| Durability | Washable and reusable | Must be reapplied |
| Visibility | Noticeable under clothing | Dries clear; can wear makeup over |
Pressure Garment Therapy
For keloids resulting from burns or large-scale trauma, pressure therapy is often employed. This involves wearing customized garments that exert 24–30 mmHg of pressure for 23 hours a day. While the mechanism isn't fully understood, it is believed that the pressure creates a localized state of hypoxia (low oxygen), which reduces fibroblast activity and slows collagen growth.
Advanced Dermatological Modalities: Cryotherapy and Laser Systems
When topical treatments and injections aren't enough, dermatologists may turn to energy-based or temperature-based interventions. These provide a more aggressive keloid treatment without surgery by physically altering the scar tissue.
Efficacy of Cryotherapy as a Keloid Treatment Without Surgery
Cryotherapy involves the application of liquid nitrogen to "freeze" the scar tissue. This causes localized cell death (necrosis) and destroys the microvasculature that feeds the keloid.
- Success Rates: Studies show a 30% to 75% success rate after two or three sessions.
- Best For: Small, recent keloids, particularly those on the earlobes or from acne.
- Side Effects: The primary risk is permanent hypopigmentation (skin lightening), as the cells that produce pigment (melanocytes) are very sensitive to cold.
Laser Systems: PDL and Fractional CO2
Lasers target the blood vessels within the keloid to starve it of nutrients.
- Pulsed-Dye Laser (PDL): This is the most common laser for scars. It targets hemoglobin to reduce the redness and itchiness of the keloid.
- Fractional CO2 Laser: This creates microscopic columns of injury in the scar to encourage more organized remodeling of the tissue.
Clinical consensus suggests that lasers are most effective when used as an adjunct. For example, using a laser to "prime" the scar can improve the penetration of subsequent steroid injections. For those interested in the technical specifics, more info about laser for keloids explores how different wavelengths interact with scar tissue.
Investigating Superficial Radiation as a Keloid Treatment Without Surgery
While the word "radiation" can be intimidating, Superficial Radiation Therapy (SRT) is a highly localized, low-depth treatment that does not penetrate to internal organs. It specifically targets the overactive fibroblasts in the skin.
SRT is most commonly used immediately following a surgical excision to prevent the scar from returning. This "sandwich" approach—surgery followed by SRT-100™ therapy—has a cure rate of more than 90%. By inhibiting the mitosis (cell division) of fibroblasts during the critical 24-48 hour window after an injury, SRT drops the recurrence rate from nearly 100% (with surgery alone) to below 10%.
Clinical Evaluation of Topical Botanical Extracts and Alternative Therapies
The internet is full of "miracle cures" for keloids, ranging from kitchen staples to essential oils. However, as a science-based resource, it is important to separate anecdotal evidence from clinical reality.
Allium Cepa (Onion Extract)
Onion extract contains quercetin, a flavonoid with anti-inflammatory and anti-proliferative properties. A 2012 study found that onion extract gel could reduce scar height and pigmentation. While not as potent as silicone or steroids, it is often included in over-the-counter scar creams as a supportive ingredient.
Aspirin Paste
Some clinical studies have explored topical aspirin. Because aspirin inhibits prostaglandin E2, it may prevent scar-promoting cells from entering the keloid site. A common home-care suggestion involves crushing 3-4 aspirin tablets and mixing them with water to form a paste, applied for 1-2 hours daily. While preliminary data is interesting, it should not replace professional medical care.
Garlic and Honey
- Garlic: Some research suggests garlic enzymes may block the substances that contribute to tissue buildup. However, raw garlic is highly caustic and can cause chemical burns on the skin if left too long.
- Honey: Raw organic honey has well-documented anti-inflammatory properties, but there is limited high-quality evidence that it can significantly flatten an established, dense keloid.
While these remedies may offer mild symptomatic relief (reducing itch or redness), they are rarely sufficient for complete keloid removal. You can stay updated on the latest peer-reviewed findings by checking more info about keloid scar research.
Clinical Considerations and Patient Inquiries in Non-Surgical Keloid Management
How long does it take to see results from non-surgical treatments?
Patience is the most important "ingredient" in any scar treatment plan. Most non-surgical interventions, such as silicone sheeting or steroid injections, require 3 to 6 months of consistent application before significant flattening or softening is observed. Clinical results are measured in months, not days.
Can keloids be permanently removed without surgical excision?
In many cases, yes. Through a combination of cryotherapy, injections, and laser treatments, a keloid can be flattened to the point where it is flush with the skin and asymptomatic. However, because the genetic predisposition remains, there is always a risk of recurrence if the area is re-injured.
What are the primary side effects of intralesional steroid therapy?
The most common side effects are localized. These include skin atrophy (thinning of the skin), telangiectasia (visible small blood vessels), and hypopigmentation (lightening of the skin color). These effects are often reversible once treatment stops, but they must be monitored by a dermatologist.
Conclusion and Clinical Outlook
Managing a keloid is often a marathon rather than a sprint. The high recurrence rate of surgery alone makes keloid treatment without surgery the logical first-line approach for the majority of patients. Whether through the occlusion of silicone gel, the anti-inflammatory power of corticosteroids, or the precision of laser and radiation therapy, modern dermatology offers numerous ways to manage these "piercing problems."
The most successful outcomes almost always involve a multimodal approach—using two or more treatments in tandem to attack the scar from different biological angles. If you are struggling with a persistent scar, the first step is a professional evaluation to determine your specific risk factors. You can start your scar assessment today to better understand your options and begin the journey toward smoother skin.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Arno, A. I., Gauglitz, G. G., Barret, J. P., & Jeschke, M. G. (2014). Up-to-date approach to manage keloids and hypertrophic scars: A useful guide. Burns, 40(7), 1255–1266. https://pubmed.ncbi.nlm.nih.gov/24767715/
- Gauglitz, G. G., Korting, H. C., Pavicic, T., Ruzicka, T., & Jeschke, M. G. (2011). Hypertrophic Scarring and Keloids: Pathomechanisms and Current and Emerging Treatment Strategies. Molecular Medicine, 17(1–2), 113–125. https://pmc.ncbi.nlm.nih.gov/articles/PMC3022978/
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/
- Gold, M. H., et al. (2014). Updated international clinical recommendations on scar management: Part 2. Dermatologic Surgery, 40(8), 825–831. https://pubmed.ncbi.nlm.nih.gov/25068544/
- Puri, N., & Talwar, A. (2009). The efficacy of silicone gel for the treatment of hypertrophic scars and keloids. Journal of Cutaneous and Aesthetic Surgery, 2(2), 104–106. https://pmc.ncbi.nlm.nih.gov/articles/PMC2918339/