Chemical Peel for Leg Scars That Actually Deliver Results
Chemical peels can resurface leg scars by removing damaged skin layers. Learn which acid types and peel depths deliver the best results for leg scarring.

Do Chemical Peels Work on Leg Scars
Chemical peel for leg scars is one of the most clinically studied resurfacing approaches for reducing the appearance of post-acne marks, hyperpigmentation, and shallow atrophic scarring on the lower extremities.
Before going further, here is a quick-reference summary for those evaluating peel options for leg scars:
| Factor | Key Clinical Point |
|---|---|
| Best peel depth for leg scars | Superficial to medium-depth (TCA 10–30%, glycolic, lactic) |
| Scar types that respond best | Atrophic acne scars, post-inflammatory hyperpigmentation, shallow traumatic scars |
| Typical sessions needed | 3–6 treatments spaced 2–6 weeks apart |
| Average recovery time | Superficial: 1–7 days; Medium: 7–14 days |
| Key risk to monitor | Post-inflammatory hyperpigmentation, especially in darker skin tones (Fitzpatrick IV–VI) |
| Insurance coverage | Generally not covered — considered cosmetic |
| Deep peels on legs | Not typically recommended due to higher complication risk on body skin |
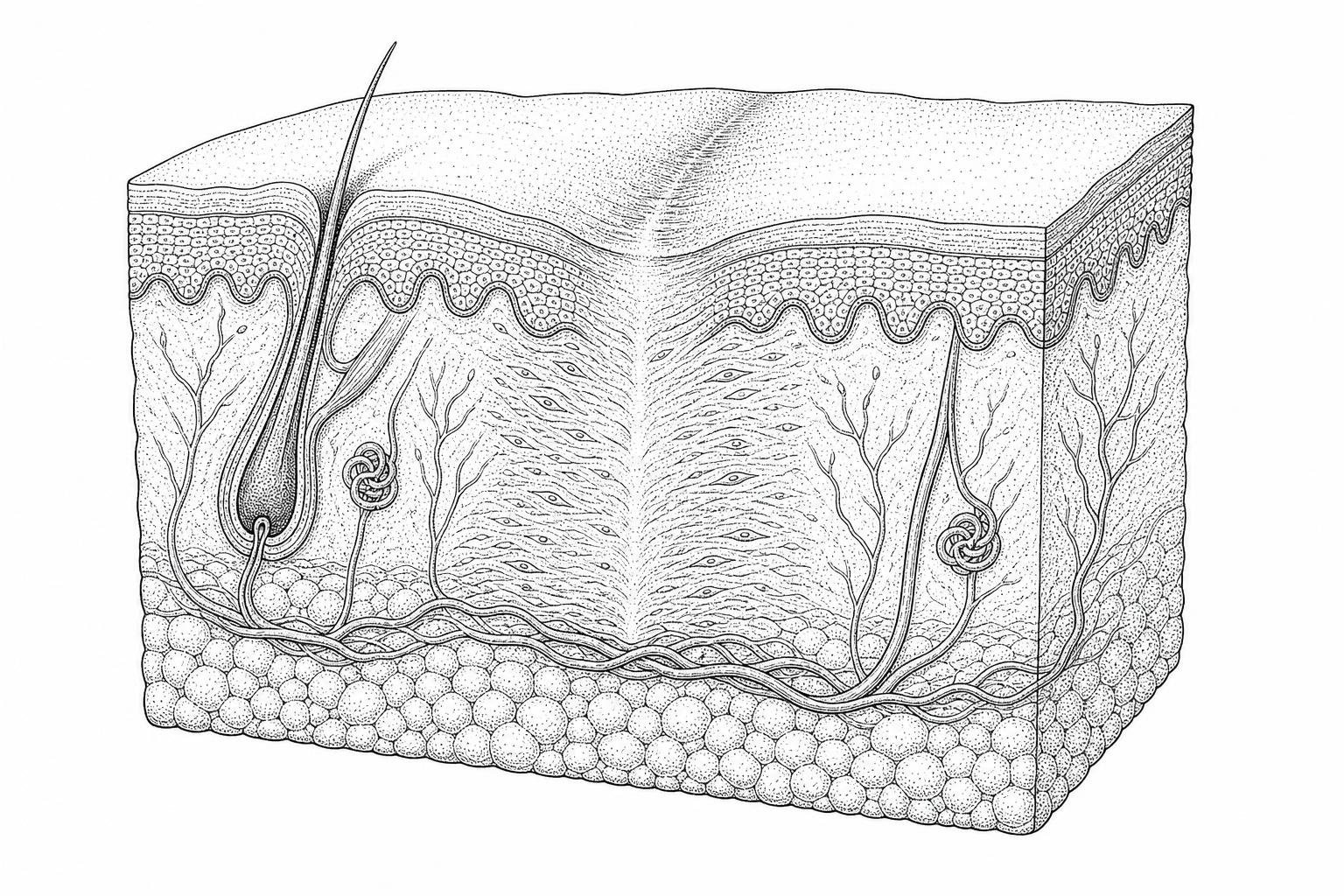
Leg skin differs meaningfully from facial skin. It is thicker, has lower follicular density, and heals more slowly — all factors that influence both acid selection and recovery expectations. Research indicates that these physiological differences require higher acid concentrations or repeated sessions to achieve comparable results to facial resurfacing.
The mechanism is well-established: a chemical solution causes controlled, graded injury to the outer skin layers. This triggers the skin's natural repair response — fibroblast activation, collagen synthesis, and epidermal turnover — gradually replacing damaged tissue with smoother, more evenly pigmented skin. As the American Society for Dermatologic Surgery notes, chemical peels improve scar appearance by removing the outer layer of old skin, with new skin typically smoother and less irregular.
What this article covers: the biology behind how peels modify scar tissue on the legs, how to select the right acid and depth, what clinical evidence shows for specific acids like TCA and glycolic acid, and how peels compare to energy-based alternatives.

This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Explore more about chemical peel for leg scars:
How Chemical Peels Resurface Leg Scars
The efficacy of a chemical peel for leg scars relies on the principle of controlled chemot exfoliation. When a chemical agent is applied to the skin, it initiates a sequence of biological events designed to replace disorganized scar tissue with a more uniform dermal matrix.
Controlled Injury and Protein Denaturation
At the molecular level, chemical peels work through protein denaturation. Acids like Trichloroacetic Acid (TCA) cause the proteins in the epidermis and dermis to coagulate. This process is often visible during clinical application as "frosting," a white precipitate that indicates the depth of penetration. This controlled injury serves as a biological signal to the body that the existing tissue is damaged and needs replacement.
How Peels Dissolve Damaged Skin Cells
Superficial peels, such as those utilizing alpha-hydroxy acids (AHAs), primarily target the stratum corneum. By inducing keratinolysis—the breakdown of the bonds between skin cells—these peels accelerate epidermal turnover. For leg scars characterized by hyperpigmentation or rough texture, this rapid shedding of dead cells helps to lift pigment and smooth the surface. This is a foundational step in Chemical Peel for Scars: Complete Guide.
How Peels Activate Skin Cell Renewal
The most significant changes in scar architecture occur in the dermis. The controlled trauma induced by medium-depth peels stimulates fibroblasts, the primary cells responsible for collagen production. Clinical evidence suggests that this stimulation leads to the synthesis of new Type I and Type III collagen fibers. Over a series of treatments, this new collagen fills in the depressions found in atrophic scars, a process known as dermal remodeling.
Glycosaminoglycan Deposition
Beyond collagen, chemical resurfacing increases the deposition of glycosaminoglycans (GAGs), such as hyaluronic acid, within the extracellular matrix. These molecules are essential for skin hydration and volume. Increased GAG levels contribute to epidermal thickening, which can make shallow scars appear less prominent by improving the overall "plumpness" of the surrounding skin.

What Determines Peel Depth on Leg Scars
Choosing the correct depth for a chemical peel for leg scars is critical because the skin on the legs is physiologically distinct from facial skin. The legs have a thicker stratum corneum but a significantly lower density of hair follicles and sebaceous glands. Since re-epithelialization (the growth of new skin) occurs largely from these follicular units, the legs heal more slowly and are more prone to scarring if a peel penetrates too deeply.
Comparing Peel Depths for Body Skin
| Peel Depth | Target Layer | Primary Ingredients | Best For |
|---|---|---|---|
| Superficial | Stratum corneum to basal layer | Glycolic (30-50%), Salicylic, Lactic | Hyperpigmentation, Keratosis Pilaris, mild texture issues |
| Medium | Papillary to upper reticular dermis | TCA (15-35%), Jessner’s Solution | Atrophic scars, sun damage, deep pigment |
| Deep | Mid-reticular dermis | Phenol, High-conc TCA (>40%) | Rarely used on legs due to high risk of permanent scarring |
Skin Thickness and Healing Capacity
The thickness of the skin on the legs varies between the shins, calves, and thighs. Areas with thinner skin and less underlying fat, such as the anterior tibia (shin), have a lower healing capacity and are more susceptible to complications. When considering the Best Chemical Peel for Leg Scars, clinicians must adjust the concentration and "dwell time" (how long the acid stays on the skin) based on the specific anatomical site.
Follicular Density and Recovery
Because the legs have fewer adnexal structures (hair follicles) compared to the face, the reservoir of stem cells available for skin repair is limited. This is why deep phenol peels, which are common for facial rejuvenation, are generally contraindicated for the legs. A medium-depth peel that reaches the papillary dermis is usually the therapeutic limit for safe leg scar revision.
Comparative Efficacy of Acid Formulations in the Treatment of Leg Scars
Different acids interact with leg tissue in unique ways. The choice of acid depends on whether the primary concern is pigment, texture, or scar depth. Clinical observations on leg resurfacing highlight that a "one-size-fits-all" approach is rarely effective for the diverse range of leg scars.
Trichloroacetic Acid (TCA) as a Chemical Peel for Leg Scars
TCA is widely regarded as the gold standard for medium-depth scar revision. Unlike AHAs, TCA is a self-neutralizing acid; once it reacts with the proteins in the skin, it stops penetrating. This provides a safety margin for the clinician.
- Mechanism: TCA causes protein coagulation, leading to the "frosting" effect.
- Efficacy: It is particularly effective for atrophic scars (depressed scars) because it reaches the dermis to trigger significant collagen synthesis.
- Concentration: For the legs, concentrations of 15% to 25% are commonly used in a series, while 35% is reserved for localized application on specific scars.
- Revision: TCA can be used in the "CROSS" technique (Chemical Reconstruction of Skin Scars), where high concentrations are applied only to the base of the scar, as discussed in Chemical Peel Scar Revision.
Glycolic and Lactic Acids: Superficial Chemical Peel for Leg Scars
Alpha-hydroxy acids are the preferred choice for superficial issues and for patients with sensitive skin or darker skin tones.
- Glycolic Acid: Derived from sugarcane, it has the smallest molecular size of the AHAs, allowing for deeper penetration. It is excellent for improving the texture of "strawberry legs" and reducing the appearance of flat, dark marks (hyperpigmentation).
- Lactic Acid: Derived from milk, lactic acid is a larger molecule and acts as a humectant. It is often used for scar treatment in patients with dry or sensitive leg skin, as it provides exfoliation while simultaneously increasing skin hydration.
- Clinical Goal: These acids work by reducing corneocyte cohesion, allowing the skin to shed more efficiently. While they do not fill deep scars as effectively as TCA, they are vital for evening out skin tone and preparing the skin for deeper treatments.
Selecting the Best Chemical Peel for Leg Scars for Darker Skin Tones
For individuals with darker skin tones (Fitzpatrick types IV-VI), the primary risk associated with chemical peels is post-inflammatory hyperpigmentation (PIH). When the skin is injured too deeply or too quickly, melanocytes—the cells that produce pigment—can become overactive, leading to dark patches that are harder to treat than the original scar.
Mandelic acid is frequently recommended as the best chemical peel for leg scars on sensitive or dark skin. It has a molecular size approximately twice that of glycolic acid. This larger structure ensures slower, more uniform penetration, which significantly reduces the risk of irritation and PIH. Research indicates that mandelic acid also has antibacterial properties and can down-regulate melanocytes, making it an ideal choice for treating "exotic" skin tones or hyperpigmented scars on the legs. Lactic acid is another safe alternative, as it is a natural humectant that exfoliates while maintaining the skin's moisture barrier.
Comparative Analysis of Chemical Resurfacing and Energy-Based Modalities
When evaluating a chemical peel for leg scars, patients often compare the procedure to laser therapy. Both aim to resurface the skin, but they use different modalities to achieve that goal.
Ablative vs. Non-Ablative
Fractional CO2 lasers are often considered the "gold standard" for deep scarring, but they carry a higher price point and significant downtime. Chemical peels, particularly medium-depth TCA peels, offer a more cost-effective alternative with a different risk profile. While lasers use light energy to create micro-channels of injury, peels use a chemical reaction to remove entire layers of skin.
Post-Inflammatory Hyperpigmentation (PIH) Risks
One of the primary concerns with any resurfacing treatment on the legs is PIH. Because the legs have slower circulation and are frequently exposed to the sun, the risk of developing dark spots after a treatment is higher than on the face. Evidence-based guide to leg skin recovery notes that chemical peels, when performed correctly with proper pre-treatment, may actually carry a lower risk of PIH for certain skin types compared to high-heat lasers.
Cost-Benefit and Accessibility
Chemical peels are generally more accessible than laser therapy. They do not require expensive machinery, making the per-session cost lower. However, achieving results comparable to a single laser session may require 3 to 4 medium-depth peels.
Standardized Clinical Protocols: Pre-Treatment Optimization and Post-Operative Management
The success of a chemical peel for leg scars is often determined before the acid even touches the skin. Proper preparation and aftercare are essential to minimize the risk of scarring and infection.
Pre-Treatment: Retinization and Tyrosinase Inhibitors
To ensure even penetration of the peel, clinicians often recommend a "pre-peel" regimen for 2 to 4 weeks:
- Retinoids: Topical tretinoin or retinol helps to thin the stratum corneum and accelerate healing.
- Tyrosinase Inhibitors: Ingredients like hydroquinone, kojic acid, or azelaic acid suppress melanin production. This is crucial for preventing PIH, especially in patients with darker skin tones.
- Antiviral Prophylaxis: For patients with a history of shingles or herpes simplex, a prophylactic antiviral may be prescribed to prevent a breakout during the healing phase.
The Procedure: Application and Neutralization
During the application, the clinician cleanses the skin to remove oils. The acid is applied in layers. For glycolic peels, a neutralizing agent (like sodium bicarbonate) is used to stop the reaction. For TCA, the acid self-neutralizes. The clinician monitors for "frosting"—the white appearance of coagulated proteins.
Post-Operative Care: Occlusion and Protection
After the peel, the skin barrier is temporarily compromised.
- Occlusive Emollients: Products containing petrolatum or ceramides are used to prevent transepidermal water loss (TEWL) and keep the skin moist, which is essential for cell migration and healing.
- Photoprotection: New skin is extremely sensitive to UV damage. Strict sun avoidance and the use of broad-spectrum SPF 30+ are mandatory for several months post-peel.
- No Picking: Patients must allow the skin to desquamate (peel) naturally. Forcing the skin to peel prematurely can lead to permanent scarring or infection.
Clinical Considerations and Frequently Encountered Patient Inquiries
Physiological Determinants of Recovery: Lower Extremity vs. Facial Integument
Leg skin has fewer sebaceous glands and hair follicles. On the face, these structures provide the stem cells necessary for rapid re-epithelialization. Because the legs lack this dense network, healing takes significantly longer—often 10 to 14 days for a medium peel, compared to 5 to 7 days on the face. Additionally, lower blood flow in the extremities can slow the overall regenerative process.
Contraindications for High-Concentration Chemical Resurfacing
Keloid scars—raised, thick scars that grow beyond the original wound boundary—are generally a contraindication for aggressive chemical peels. The inflammatory response triggered by a peel can potentially stimulate further keloid growth. Similarly, active infections, open wounds, or undiagnosed skin lesions should never be treated with a chemical peel.
Temporal Progression of Erythema and Desquamation
For a medium-depth chemical peel for leg scars, the timeline typically follows this pattern:
- Days 1-3: The skin feels tight and may turn a dark, brownish-red color.
- Days 4-7: Peeling (desquamation) usually begins, often starting in areas of high movement.
- Days 7-14: Peeling continues. The skin underneath may appear pink (erythema).
- Weeks 2-6: Erythema gradually fades. The full results of collagen remodeling begin to appear over the following 3 to 6 months.
How many sessions are required for significant leg scar reduction?
Clinical observations suggest a series of 3 to 6 treatments, spaced 4 to 6 weeks apart, are typically necessary for noticeable remodeling of leg scar tissue. Stubborn hyperpigmentation or older scars may require a longer maintenance plan.
Can chemical peels treat old or white (striae alba) scars on the legs?
Chemical peels are most effective for pigmented (red or brown) and superficial textural scars. Older white scars, which lack pigment and have dense, stagnant collagen, are notoriously difficult to treat with peels alone. They may require combination therapy with microneedling to stimulate new melanocyte activity.
Summary and Clinical Outlook
A chemical peel for leg scars is a scientifically validated method for improving skin texture and reducing the visibility of traumatic or acne-related scarring. By leveraging the body’s natural wound-healing response, these treatments can transform disorganized scar tissue into smoother, healthier skin. However, the unique physiology of the legs requires a cautious, evidence-based approach to acid selection and depth.
For those considering this procedure, a professional consultation is necessary to determine the specific needs of your skin type. You can begin by taking a Personalized scar treatment assessment to better understand your options. With the right clinical protocol and diligent post-operative care, chemical resurfacing remains one of the most effective tools in the field of scar revision.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Lee, K. C., Wambier, C. G., et al. (2019). Basic chemical peeling: Superficial and medium-depth peels. Journal of the American Academy of Dermatology, 81(2), 313–324. https://pubmed.ncbi.nlm.nih.gov/30550830/
- Castillo, D. E., & Keri, J. E. (2018). Chemical peels in the treatment of acne: patient selection and perspectives. Clinical, Cosmetic and Investigational Dermatology, 11, 365–372. https://pmc.ncbi.nlm.nih.gov/articles/PMC6053170/
- Fitzpatrick, T. B. (1988). The Validity and Practicality of Sun-Reactive Skin Types I Through VI. Archives of Dermatology, 124(6), 869–871. https://pubmed.ncbi.nlm.nih.gov/3377516/
- Roberts, W. E. (2004). Chemical Peeling in Ethnic/Dark Skin. Dermatologic Therapy, 17(2), 196–205. https://pubmed.ncbi.nlm.nih.gov/15113287/