The Definitive Guide to Best Burn Scar Treatments
Evidence-based guide to the most effective burn scar treatments, from silicone sheets and pressure garments to laser therapy and surgical revision.

Burn Scar Treatment: A Clinical Overview
Finding the best treatment for burn scars depends on scar type, depth, age, and location — but here is what current clinical evidence supports:
Quick-reference: Most effective burn scar treatments by evidence level
| Treatment | Best For | Evidence Level |
|---|---|---|
| Silicone gel sheets | Hypertrophic scars, early management | Strong |
| Pressure garments | Raised, active scars (first 12–18 months) | Moderate–Strong |
| Pulsed dye laser (PDL) | Redness, inflammation, vascular scars | Strong |
| Fractional CO2 laser | Stiff, thick, contracted scars | Strong |
| Corticosteroid injections | Hypertrophic scars and keloids | Strong |
| Corticosteroid + 5-FU combination | Resistant hypertrophic scars | Moderate |
| Scar massage and hydration | All scar types, early and mature | Moderate |
| Z-plasty / skin grafting | Contractures limiting movement | Strong (surgical) |
| Microneedling + PRP | Texture, pliability improvement | Preliminary |
| Stem cells / 3D bioprinting | Severe burns | Early-stage research |
Burn injuries are one of the most damaging forms of trauma the skin can experience. Approximately 11 million people worldwide require medical treatment for burns each year, and over 180,000 burn-related deaths occur annually — the vast majority in low- and middle-income countries. Among survivors, the burden does not end with wound closure.
Up to 70% of burn patients develop hypertrophic scars or contractures — raised, rigid scar tissue that can restrict movement, cause chronic pain, and significantly affect quality of life.
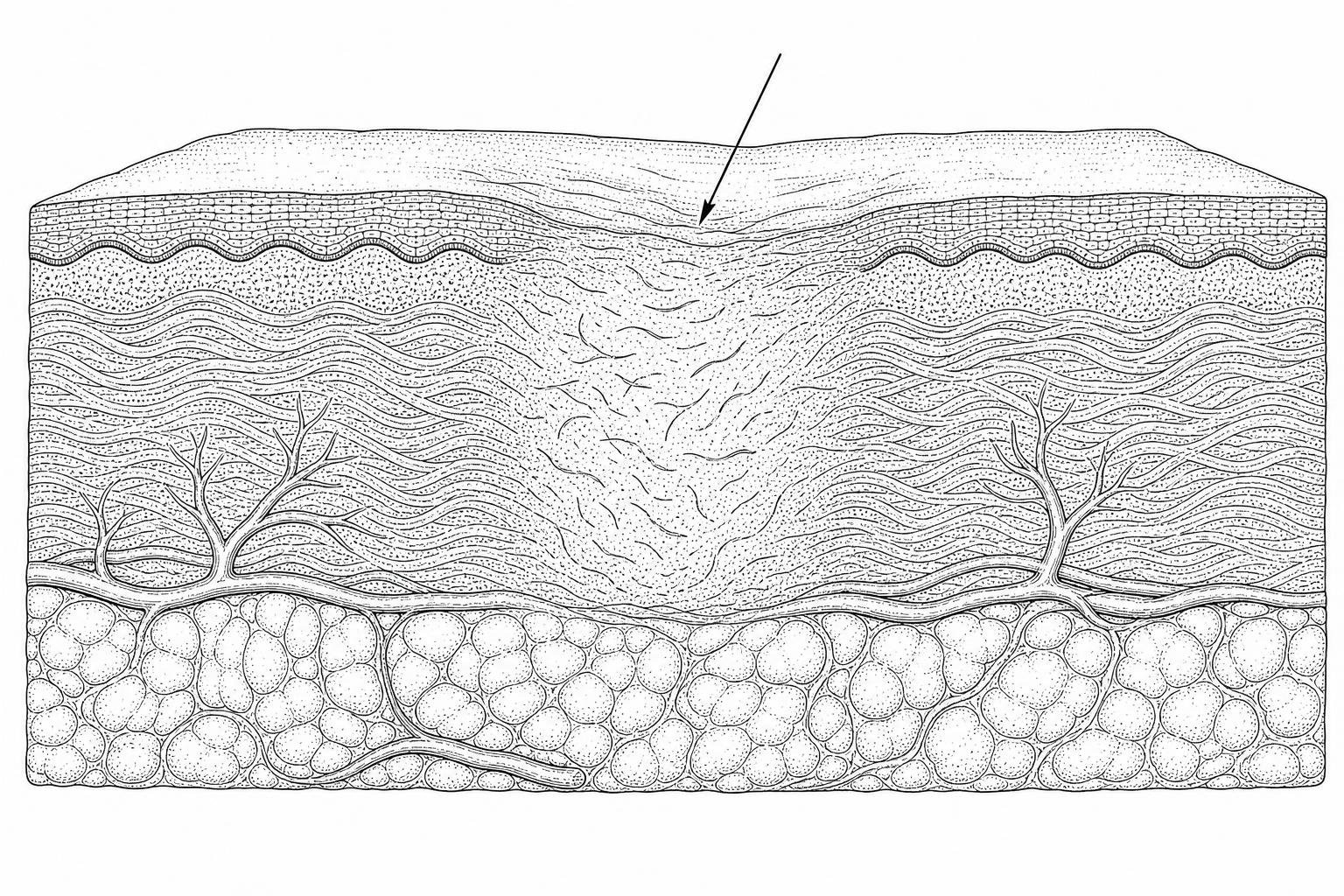
Scars form because burn injuries damage the dermis, the deep structural layer of the skin. The body responds by producing collagen rapidly, but in a disorganized pattern rather than the aligned structure of healthy skin. This abnormal collagen deposition is what creates raised, firm, or contracted scar tissue. The process typically peaks around six months after injury and continues to mature over 12 to 18 months.
The good news, as of May 2026, is that the range of clinically validated treatments has expanded considerably — from early wound care and silicone therapy to advanced laser modalities, regenerative dermal matrices, and emerging cellular therapies. No single treatment works for every scar, but a structured, evidence-based approach can meaningfully improve both appearance and function.
This guide reviews the full spectrum of options, from what to do in the first days after a burn through to surgical reconstruction and long-term scar management.
How burn scars form

The clinical outcome of a burn injury is primarily determined by its depth. Burns are classified by how many layers of skin they penetrate. First-degree burns affect only the epidermis (the top layer) and typically heal within a week without scarring. Second-degree, or partial-thickness burns, extend into the dermis. If these heal in less than 14 days, scarring is usually minimal; however, if healing takes longer, the risk of problematic scarring increases significantly. Third-degree, or full-thickness burns, destroy both the epidermis and the entire dermis, often requiring surgical intervention and resulting in permanent scars.
Within the burn site, clinicians identify three distinct zones: the zone of coagulation (the center where tissue is lost), the zone of stasis (surrounding tissue with reduced blood flow), and the zone of hyperemia (the outermost area that usually recovers). Research published in the Annals of Plastic Surgery suggests that the zone of stasis is a critical therapeutic target; preserving this tissue through early intervention can reduce the total area of permanent scarring.
How Burn Scar Classification Guides Treatment
Burn scars are categorized into three main types, each requiring a different management strategy:
- Hypertrophic Scars: These are raised, red, and itchy. They stay within the boundaries of the original wound and often develop within weeks of the injury.
- Keloid Scars: These grow beyond the original wound edges. They are more common in individuals with darker skin tones and can be difficult to treat due to high recurrence rates.
- Contractures: These occur when scar tissue tightens, pulling the skin edges together. This often happens over joints, significantly restricting movement.
Clinicians use standardized tools like the Vancouver Scar Scale (VSS) and the Patient and Observer Scar Assessment Scale (POSAS) to quantify scar height, pliability, and vascularity, helping to determine the best treatment for burn scars for each individual.
Why burn scars form and thicken
The development of a burn scar is a biological process driven by complex cellular signals. Transforming growth factor-beta 1 (TGF-β1) and interleukin-6 (IL-6) are key proteins that signal fibroblasts to transform into myofibroblasts. These specialized cells "contract" the wound and pump out excessive amounts of collagen.
The maturation timeline is a critical factor in treatment. Scarring usually peaks around 6 months post-injury, characterized by redness and firmness. Over the following 12 to 18 months, the scar "matures," often becoming flatter and softer. Understanding this timeline prevents premature surgical intervention when non-surgical options may still be effective.
Clinical Evidence for Burn Scar Therapies

Prevention is often the most effective strategy. Research indicates that maintaining a moist wound environment and preventing infection are the first steps in minimizing scar formation. Dermatologists often recommend applying petroleum jelly to new wounds to prevent scabbing, which can slow the healing process. For larger burns, specialized dressings are used to maintain hydration and protect the fragile new skin.
Evidence-Led Review of Silicone and Pressure Therapy
For decades, silicone therapy and pressure garments have been the "gold standard" for non-surgical scar management.
- Silicone Gel Sheets: Clinical guidelines suggest wearing silicone sheets for 12–24 hours a day for at least 2 to 3 months. The silicone works by increasing the hydration of the stratum corneum, which signals the body to downregulate collagen production.
- Pressure Therapy: Custom-fitted garments that apply 15–25 mmHg of pressure are used to physically realign collagen fibers and reduce blood flow to the scar, which helps flatten it. This is most effective when started early and worn consistently for several months.
Detailed protocols for these methods can be found in our non-surgical burn scars complete guide.
For a deeper comparison of silicone formulations by skin type, see our guide to the best scar creams with silicone. If you're managing a hypertrophic scar specifically, our silicone gel for hypertrophic scars review covers the clinical protocols in detail.
The Role of Massage and Topical Hydration
Once the wound has closed, massage and hydration become essential. Circular massage techniques performed several times daily can help break up dense collagen bundles and improve the pliability of the tissue.
Topical emollients, particularly those containing hyaluronic acid, help maintain the skin barrier. It is vital to avoid moisturizers with fragrances or high alcohol content, as burned skin is highly sensitive and prone to irritation. Emerging evidence also suggests that deficiencies in Vitamin C and D can impair the quality of the skin's remodeling phase, highlighting the role of nutrition in recovery.
Do lasers work on burn scars?
The last decade has seen a dramatic shift in how we treat mature burn scars, thanks to advancements in laser technology. According to Johns Hopkins Medicine, laser therapy has moved from a cosmetic option to a functional necessity.
Comparing lasers for burn scars
Different lasers target different aspects of the scar:
- Pulsed Dye Laser (PDL): Operating at a 595 nm wavelength, this laser targets the blood vessels within a scar. By cauterizing these vessels, it reduces the redness and inflammation that drive scar growth.
- Fractional CO2 Laser: This laser creates microscopic "holes" in the scar tissue. This process, known as fractional resurfacing, allows the stiff, thick tissue to become more flexible. It is particularly effective for improving the range of motion in scars that have become rigid.
Beyond appearance, these lasers provide significant relief from "pruritus" (intense itching) and neuropathic pain. In many cases, insurance now covers these treatments when they are used to restore functional movement.
For a full breakdown of CO2 laser efficacy data, see our CO2 laser for acne scars guide. For surgical scar results specifically, see CO2 laser for surgical scars: before and after. Patients with darker skin tones should also read our laser scar removal for dark skin guide.
Microneedling and injections for burn scars
When lasers or silicone aren't enough, adjunct therapies can provide targeted relief. Corticosteroid injections are frequently used to flatten thick hypertrophic scars and keloids. Some specialists combine these with 5-Fluorouracil (5-FU), a chemotherapy agent that further inhibits the overactive fibroblasts.
Microneedling is also gaining traction, not just for its ability to stimulate healthy collagen, but as a delivery mechanism for topical medications. Platelet-Rich Plasma (PRP) is sometimes used alongside microneedling to introduce growth factors that may accelerate the maturation of the scar tissue.
Our scar tissue massage therapy guide covers specific techniques and pressure protocols. For more on microneedling as a standalone treatment, see microneedle scar removal: the ultimate guide.
Surgical options for severe burn scars
When a scar causes a functional contracture—meaning you cannot fully move a joint or limb—surgery becomes the necessary best treatment for burn scars. Johns Hopkins Medicine notes that while surgery cannot completely remove a scar, it can "exchange" a problematic scar for one that is thinner and more flexible.
Advanced Dermal Matrices and Cellular Therapies
Modern surgery often utilizes regenerative materials rather than just traditional skin grafts.
- Dermal Matrices (e.g., Integra, BTM): These act as a scaffold, allowing the body to regrow its own dermal-like tissue.
- ReCell: This technology uses a small sample of the patient's own skin to create a "spray-on" suspension of skin cells, which can cover larger areas with minimal donor site trauma.
- Mesenchymal Stem Cells: Research into stem cell therapy aims to modulate the immune response to prevent the initial formation of fibrosis.
Treating tight, restrictive burn scars
The primary goal of surgical reconstruction is functional restoration. Techniques like Z-plasty or W-plasty involve making triangular incisions to "lengthen" the scar, effectively releasing the tension over a joint. For more severe cases, skin flaps (which bring their own blood supply) or tissue expansion (using a balloon-like device to grow extra skin) may be required to provide enough healthy tissue for the repair.
For keloid-specific treatment pathways, see our keloid treatment without surgery guide and laser for keloid scars review. For a broader overview of hypertrophic scar management including surgical options, see our scar revision treatment guide.
Long-Term Management and Multidisciplinary Care
The journey of burn scar management is a marathon, not a sprint. Long-term care is vital to maintaining the results of any treatment.
The Role of Multidisciplinary Teams in Recovery
Because burn injuries affect the whole person, the best outcomes are achieved through a multidisciplinary team. This includes burn surgeons, physical and occupational therapists to maintain range of motion, and psychologists to address the psychosocial impact of scarring.
One of the most overlooked aspects of long-term care is sun protection. Healed burn scars are highly susceptible to hyperpigmentation and, more importantly, have a higher long-term risk of developing skin cancer if not protected. Applying broad-spectrum SPF 30+ every two hours when outdoors is a non-negotiable part of long-term scar care.
Frequently Asked Questions about Burn Scar Treatment
How long does it take for a burn scar to fully mature?
The maturation process typically takes 12 to 18 months. During this time, the scar will change in color from red/purple to a paler tone and gradually soften. It is generally recommended to wait until the scar is mature before considering major surgical revisions, unless the scar is causing a severe loss of function.
Can laser therapy replace the need for burn scar surgery?
In some cases, yes. Laser therapy can improve the pliability of a scar so much that surgery is no longer needed to release a contracture. Clinicians sometimes refer to this as "prehabilitation"—using lasers to soften the tissue and reduce the complexity of a future surgery.
Are silicone gel sheets more effective than silicone gels for burns?
Evidence generally suggests that silicone sheets are slightly more effective because they provide a small amount of occlusion and pressure. However, silicone gels are often preferred for the face or joints where sheets are difficult to keep in place. Consistency of use is more important than the specific format.
Conclusion
Managing a burn scar requires a combination of patience, clinical expertise, and consistent daily care. From the initial wound healing phase to advanced laser and surgical options, the goal is always the same: to restore as much function and comfort as possible. While no treatment can "erase" a scar, the evidence-based interventions available in 2026 offer more hope than ever for significant improvement.
If you are dealing with a problematic scar, the first step is a professional evaluation. Start your scar assessment today to understand which path is right for your recovery.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Abarca-Pineda, Y. A., et al. (2025). Conventional and Emerging Surgical and Non-surgical Approaches to the Management of Skin Burn Scars: A Comprehensive Review. Cureus, 17(8), e90982. https://pmc.ncbi.nlm.nih.gov/articles/PMC12460041/
- Johns Hopkins Medicine. (2020). Innovative Treatments for Scars from Burns and Other Trauma. https://www.hopkinsmedicine.org/news/articles/2020/04/innovative-treatments-for-scars-from-burns-and-other-trauma
- Tredget, E. E., Levi, B., & Donelan, M. B. (2014). Biology and Principles of Scar Management and Burn Reconstruction. Surgical Clinics of North America, 94(4), 793–815. https://pubmed.ncbi.nlm.nih.gov/25085089/
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/