The Best Ways to Handle Hypertrophic and Plastic Surgery Scars
Hypertrophic and plastic surgery scars can be improved with the right revision strategy. Explore evidence-based treatments from silicone therapy to surgical and laser-based interventions.
What Scar Revision Aims to Achieve
Scar revision treatment is a broad category of clinical interventions designed to reduce the visibility, discomfort, or functional impact of scars left behind by injury, surgery, burns, or skin conditions such as acne.
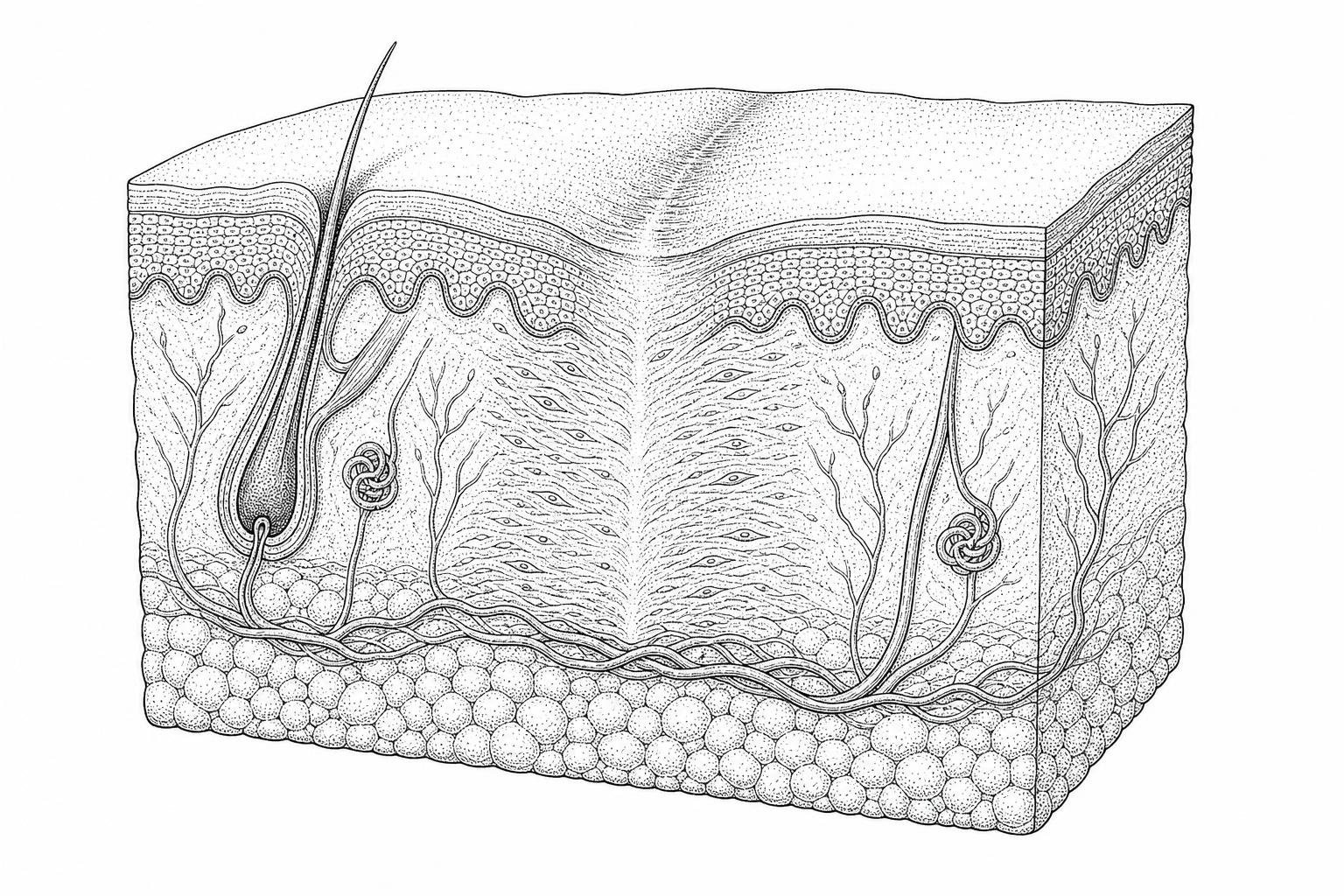
It is important to understand one key point from the outset: no treatment can completely erase a scar. Scars are permanent by nature — they form when the deeper layer of skin known as the reticular dermis is disrupted, triggering the body's wound repair cascade. What scar revision can do is meaningfully improve a scar's appearance, texture, color, and in some cases, its effect on movement.
Common scar revision options, at a glance:
| Treatment Category | Examples | Best Suited For |
|---|---|---|
| Topical therapies | Silicone gel, pressure therapy | Mild, newly formed, or flat scars |
| Injectable agents | Corticosteroids, 5-fluorouracil, dermal fillers | Raised scars, keloids, depressed scars |
| Resurfacing | Laser therapy, dermabrasion, chemical peels, microneedling | Surface irregularities, discoloration, texture |
| Surgical techniques | Z-plasty, W-plasty, excision, skin grafts | Severe, contracture, or functionally limiting scars |
Timing matters significantly. Clinical evidence indicates that most scars require 12 to 18 months to mature before surgical revision is appropriate — intervening too early on an immature scar tends to produce poor outcomes. For scars still in active remodeling, non-surgical adjunct therapies are generally recommended first.
The right approach depends on the scar's type, location, size, and the patient's overall health. A hypertrophic scar on the chest responds differently than a depressed acne scar on the cheek — and both require different clinical strategies.
The sections below cover the full spectrum of evidence-based scar revision methods, from the biology of scar formation through to advanced surgical correction.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
The Science Behind Scar Revision
Understanding the biological foundation of wound healing is essential for determining the appropriate timing and method of scar revision treatment. The human body repairs skin through a complex, three-phase process: the inflammatory phase (lasting 2 to 5 days), the proliferative phase (where new tissue is built), and the maturation phase.
During maturation, the body reorganizes collagen fibers. This phase is critical because it dictates the final texture and strength of the tissue. Clinical research suggests that it takes approximately 12 to 18 months for a scar to fully mature and reach its maximum tensile strength, which is generally only 70% to 80% of uninjured skin.
A primary objective of any revision is to ensure the treatment aligns with these biological windows. For example, Scientific research on scar revision emphasizes that immature scars—those that are still red, itchy, or elevated—often respond poorly to surgical intervention. Instead, clinicians utilize a scar assessment to evaluate parameters such as vascularity, pigmentation, pliability, and height before proceeding.
Permanent scarring occurs when the reticular dermis, the lower layer of the dermis containing dense connective tissue, is violated. If the injury is superficial (epidermal), the skin may regenerate without a trace. However, when the reticular dermis is involved, the resulting fibrous tissue lacks the organized structure of original skin, leading to the various types of scars addressed in clinical practice.

Patient Selection Criteria
Not every individual with a scar is an immediate candidate for revision. Patient selection is a rigorous process involving the evaluation of metabolic health and lifestyle factors that directly impact wound healing.
Two of the most critical physiological requirements for surgical candidates are:
- Smoking Cessation: Patients must be smoke-free for at least 30 days before and after a procedure. Tobacco use causes vasoconstriction and impairs oxygen delivery to healing tissues, significantly increasing the risk of necrosis or wound dehiscence.
- Glycemic Control: For those with diabetes, blood glucose levels should ideally be less than 180 mg/dL. Elevated glucose interferes with collagen cross-linking and increases the risk of surgical site infections.
Furthermore, following post-surgery care instructions is a prerequisite for a successful outcome. Candidates must have realistic expectations, acknowledging that the goal is to diminish, not eliminate, the mark.
Pathogenesis of Proliferative Scars
Proliferative scars, specifically hypertrophic and keloid scars, result from an aberration in the healing process where fibroblast activity becomes overactive. This leads to an overproduction of collagen within the extracellular matrix.
- Hypertrophic Scars: These are raised, red, and thick, but they remain within the boundaries of the original wound. They often improve naturally over a year or more.
- Keloid Scars: These are more aggressive, extending beyond the edges of the original injury. They are characterized by chronic inflammation in the reticular dermis.
Managing these types of tissue requires specific strategies, such as the hypertrophic scar management techniques used to break up dense collagen bundles. Genetic predisposition plays a significant role in keloid formation, and recurrence is a major clinical challenge, often requiring a combination of surgery and adjunct therapies.
Non-Surgical Treatments and Skin Resurfacing
Non-surgical interventions are often the first line of defense, especially for scars that are less than one year old or for patients seeking to avoid the risks of the operating room.
| Modality | Mechanism of Action | Clinical Application |
|---|---|---|
| Silicone Therapy | Hydrates the stratum corneum; reduces fibroblast activity. | Hypertrophic scars; prevention. |
| Pressure Therapy | Induces localized hypoxia; reduces collagen synthesis. | Keloids; burn scars (4-6 months use). |
| Corticosteroids | Inhibits inflammatory mediators and collagen production. | Raised, itchy, or painful scars. |
Intralesional injections of triamcinolone acetonide are a staple in scar revision treatment. Typically, 0.1 mL is injected per 5 to 8 mm of a linear scar every four weeks. While effective, up to 63% of patients report adverse effects such as skin atrophy or telangiectasia. Another potent agent is 5-fluorouracil (5-FU), an antimetabolite that stops cell growth in overactive scar tissue.
For those exploring non-invasive keloid removal, cryotherapy—the application of extreme cold to freeze and destroy scar tissue—is an option, though it carries a risk of pigment changes.
Resurfacing techniques like microneedling for scar reduction and chemical peel scar revision work by creating controlled micro-injuries or exfoliating the top layers of skin. This stimulates the body to produce new, more organized collagen and elastin, improving the overall texture and blending the scar with surrounding healthy skin.
Laser-Based Modalities
Laser technology has transformed the field by allowing for precise targeting of specific scar components.
- Pulsed Dye Laser (PDL): Targets hemoglobin to reduce the redness (vascularity) of a scar. This is particularly effective for red scar fading.
- Ablative Lasers (CO2 and Erbium:YAG): These lasers remove thin layers of skin and induce collagen remodeling. They are often used for laser for keloid scars or to smooth out surgical incisions.
- Fractional Photothermolysis: This creates microscopic columns of thermal damage, leaving surrounding tissue intact to speed up healing.
Injectable Fillers and Regenerative Agents
For depressed or atrophic scars—common after acne or chickenpox—the goal is to restore lost volume. Hyaluronic acid fillers provide immediate results that can last from three months to a full year. In more complex cases, atrophic scar therapy may involve subcision (breaking the fibrous bands under the scar) combined with fillers.
A more permanent solution is autologous fat grafting. This involves harvesting fat cells from one part of the body and injecting them beneath the scar. Research indicates that adipose-derived stem cells within the fat graft may have regenerative potential, improving the skin's quality beyond simple volume replacement.
Surgical Methodologies for Structural and Functional Scar Correction
When a scar is severe, restricts movement, or is poorly oriented, surgical scar revision treatment becomes necessary. The primary goal of surgery is to rearrange the tissue so the scar follows the Relaxed Skin Tension Lines (RSTLs)—the natural creases of the skin.
One of the most common techniques is the Z-plasty. This involves creating triangular flaps of skin that are transposed to change the direction of the scar and release tension. For example, a Z-plasty at a 60-degree angle can lengthen a scar by 75% and change its direction by 90 degrees.
Other techniques include:
- Fusiform Elliptical Excision: The scar is cut out in an oval shape. To ensure a flat result, surgeons use a 3:1 length-to-width ratio with end angles no more than 30 degrees.
- W-plasty and Geometric Broken-Line Closure (GBLC): These methods break a long linear scar into an irregular pattern, making it harder for the human eye to track and reducing the risk of contracture.
After these procedures, surgical scar laser treatment may be used as an adjunct to further refine the surface.
Skin Grafting and Flap Surgery for Contractures
For extensive scars, such as those from severe burns or certain abdomen scar reduction cases, simple excision is impossible due to a lack of healthy local tissue.
- Skin Grafting: A thin layer of skin is taken from a donor site (like the thigh) and placed over the wound. While functional, grafts may not perfectly match the color or texture of the surrounding skin.
- Flap Surgery: This is more complex, moving a full thickness of skin along with its own blood supply (fat, vessels, and sometimes muscle). Flaps generally provide better cosmetic and functional outcomes than grafts.
- Tissue Expansion: A silicone balloon is inserted under healthy skin and gradually inflated with saline over several weeks. This stretches the skin, creating "extra" tissue that can be used to replace the scarred area.
According to the MedlinePlus medical encyclopedia, these methods are vital for restoring functional movement in areas where scar contracture has "pulled" the skin tight, such as over joints.
Perioperative Management, Risk Assessment, and Post-Treatment Recovery
The success of scar revision treatment is heavily dependent on the patient's adherence to clinical protocols.
Pre-operative Preparation:
- Nutrition: A diet rich in protein, zinc, and vitamins A, C, and E is recommended to support the proliferative phase of healing.
- Medication Management: Patients must stop taking anticoagulants (blood thinners) as advised by their provider to minimize hematoma risk.
Potential Risks: All surgical procedures carry risks, including infection, bleeding, and adverse reactions to anesthesia. Specific to scar revision, there is a risk of the scar returning (recurrence), wound separation, or hyperpigmentation. Up to 75% of patients undergoing certain intensive treatments like intralesional cryotherapy report some form of adverse effect, highlighting the need for careful consultation.
Recovery and Long-Term Outlook: Recovery varies by treatment. Topical treatments require months of daily use (12–24 hours a day). Surgical recovery may take weeks for initial healing, but the final result will not be visible for a full year.
During this time, knowing when to apply scar cream and performing scar tissue massage can help keep the tissue pliable. Sun protection is mandatory; UV exposure can permanently darken a healing scar, a process known as post-inflammatory hyperpigmentation.
Clinical Inquiries and Patient Considerations
Timing of Clinical Intervention
Most clinicians recommend waiting at least 12 to 18 months. This allows the scar to undergo full collagen remodeling and "soften." Intervening on an immature, red scar can lead to increased inflammation and a worse aesthetic outcome.
Limitations of Surgical Correction
Surgical intervention replaces one scar with another, hopefully thinner and better-positioned one. The goal of scar revision treatment is to make the mark less conspicuous and more functional, not to restore the skin to its pre-injury state.
Risk Factors for Keloid Recurrence
The most significant risk is recurrence. Keloids have a high tendency to return, sometimes larger than the original. To combat this, surgeons often combine excision with corticosteroid injections or pressure therapy for several months post-surgery.
Summary of Evidence-Based Scar Management
Effective scar management requires a multidisciplinary approach tailored to the specific biology of the tissue. Whether utilizing non-invasive topicals or advanced surgical maneuvers, the priority of scar revision treatment remains consistent: improving the patient's quality of life through evidence-based care. By utilizing scar assessment tools and adhering to strict pre- and post-operative guidelines, significant improvements in both form and function are achievable.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Son, D., & Harijan, A. (2014). Overview of Surgical Scar Prevention and Management. Journal of Korean Medical Science, 29(6), 751–757. https://pmc.ncbi.nlm.nih.gov/articles/PMC4055805/
- Garg, S., & Dahiya, N. (2014). Surgical scar revision: An overview. Journal of Cutaneous and Aesthetic Surgery, 7(1), 3–13. https://pubmed.ncbi.nlm.nih.gov/24761092/
- Block, L., & King, T. W. (2023). Scar Revision. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK542318/
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/