The Best Scar Creams with Silicone for Every Skin Type
Silicone-based scar creams are among the most studied topical treatments in dermatology. Learn what the clinical evidence says about choosing the right silicone formula for your skin type.

Does Silicone Scar Cream Actually Work
The question most readers are asking is straightforward: what does clinical evidence say about the best scar cream with silicone? Current dermatology and scar-management guidelines generally regard topical silicone - used as a gel or sheet - as a first-line non-invasive option for preventing and treating hypertrophic scars and, in some cases, keloids. Evidence is stronger for raised surgical and traumatic scars than for atrophic acne scars.
For quick orientation, the evidence-based options can be summarized as follows:
| Scar Type | Recommended Silicone Format | Evidence Level |
|---|---|---|
| Hypertrophic (raised) scars | Silicone gel or sheeting | Moderate |
| Keloid scars | Silicone gel or sheeting | Low to moderate |
| Post-surgical scars | Self-drying silicone gel | Moderate |
| Facial / eyelid scars | Medical-grade silicone gel | Limited to moderate |
| Acne scars | Silicone gel | Limited evidence |
| Old / mature scars | Silicone gel with extended use | Low to moderate |
Practical points supported by clinical practice and published reviews include:
- Look for products listing silicone compounds such as polysiloxanes or dimethicone among the main ingredients.
- Medical-grade formulations are generally preferred in clinical settings because they are designed to form a consistent, durable film.
- Gels are usually easier to use on the face, joints, and other irregular surfaces than sheeting.
- Improvement requires consistent use over months. Research reviews suggest visible changes often emerge gradually over 2 to 6 months, with some studies following patients for longer.
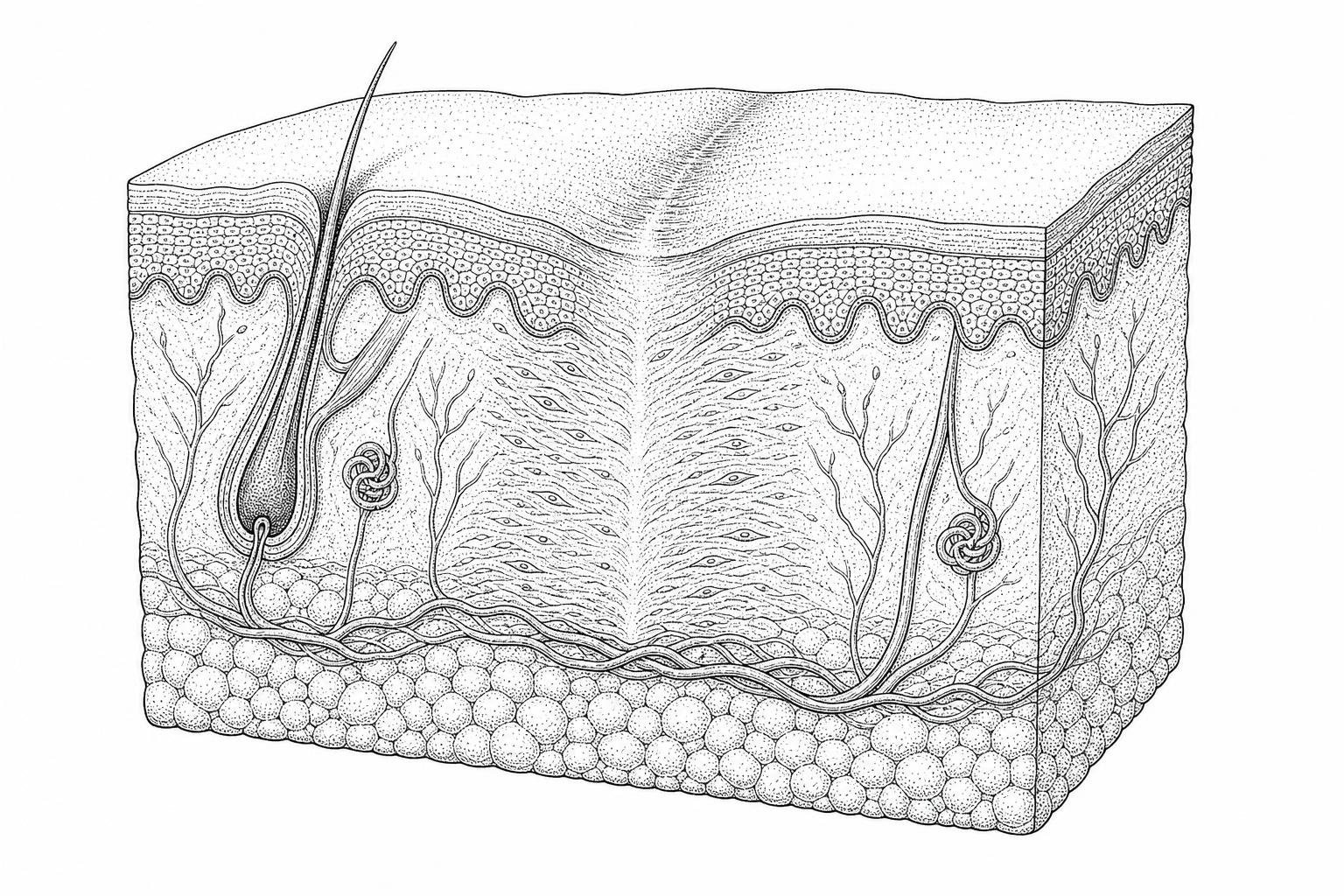
Scars form when an injury extends into the dermis, the deeper structural layer of skin. During healing, fibroblasts produce collagen rapidly to restore tissue continuity. That collagen is not arranged exactly like uninjured skin, so the healed area may become raised, firm, discolored, or texturally different.
For many people, scars on visible areas such as the face or neck carry a real psychological burden. The available evidence does support silicone as a reasonable non-invasive first option. A Cochrane review of silicone gel sheeting found some evidence of benefit in preventing and treating hypertrophic and keloid scars, but also noted that many studies were small and at risk of bias. More recent reviews likewise suggest that topical silicone may improve scar height, pliability, and color, while emphasizing that study quality remains variable. For background on scar biology, the U.S. National Library of Medicine's NCBI Bookshelf overview of wound healing provides a useful reference.
It is important to set realistic expectations: silicone does not erase scars. It may help remodel them over time by improving hydration and supporting a more favorable healing environment, which can reduce thickness, stiffness, and discoloration in some scar types.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
How Silicone Helps Skin Repair
To understand why silicone is widely used in scar management, it helps to start with skin barrier biology. Newly formed scar tissue does not immediately function like intact skin. In particular, the stratum corneum - the outermost protective layer - is often immature, which can contribute to increased transepidermal water loss (TEWL), meaning excess evaporation of water from the skin surface.
Higher TEWL is thought to contribute to abnormal scar signaling. One proposed mechanism is that poorly hydrated scar tissue sustains fibroblast activity. Fibroblasts are the cells that produce collagen and other extracellular matrix components. In hypertrophic and keloid scars, fibroblast signaling and collagen deposition become dysregulated, leading to excessive or prolonged tissue buildup.
Topical silicone appears to work primarily through occlusion and hydration rather than deep chemical penetration. When applied as a gel or sheet, it forms a semi-occlusive barrier over the scar. Research and clinical reviews suggest this barrier may:
- Reduce TEWL: By limiting water loss, silicone helps maintain hydration in the scar surface.
- Alter fibroblast signaling: Better hydration may help normalize the biochemical environment associated with excess collagen production.
- Influence remodeling pathways: Some experimental and clinical literature suggests effects on growth factors and cytokines involved in scar formation, although these mechanisms are not fully established in humans.
This mechanistic model is plausible and is frequently cited in scar literature, but it should be described cautiously. The strongest human evidence supports the clinical effect of prolonged occlusion and hydration; the exact downstream molecular pathways, including effects on transforming growth factor beta (TGF-beta), are still being investigated.
Research reviews indicate that a hydrated, protected scar environment may help scars become flatter, softer, and less erythematous over time, especially in hypertrophic scars.
How to Choose a Silicone Scar Cream
When evaluating the best scar cream with silicone, the main criterion is whether it contains medical-grade silicone compounds that form a stable, breathable film over closed skin. Common ingredients include polysiloxanes and dimethicone, sometimes combined with silicon dioxide to improve texture and drying characteristics.
A high-quality scar reduction cream should create durable coverage without causing unnecessary irritation. Because silicone is often used on visible or acne-prone areas, the most practical formulations are typically fragrance-free and non-comedogenic, although formal comedogenicity testing is not available for every product.
Sun protection is also important. Ultraviolet exposure can worsen post-inflammatory hyperpigmentation and prolong redness in healing scars. Rather than relying on combined formulations alone, many clinicians advise applying a broad-spectrum sunscreen of at least SPF 30 over a fully dried silicone film when the scar is exposed to daylight. Guidance from organizations such as the American Academy of Dermatology supports sun protection during scar maturation.
Formulating the best scar cream with silicone for facial use
The face presents distinct challenges because the skin is more visible, often oilier, and in some areas thinner and more sensitive. Silicone gel is usually more practical than sheeting on facial scars because it conforms better to contours and is less likely to detach.
A small 2019 study published in the Journal of Cosmetic Dermatology reported reduced scar thickness after eyelid surgery with silicone-based treatment, suggesting potential benefit in this setting. However, evidence for facial and eyelid scars remains more limited than for broader hypertrophic scar management, so claims should be conservative.
Some formulations also include secondary ingredients such as allantoin or lipids intended to improve tolerability. These may help with comfort, but current evidence does not show that they are the primary reason silicone products work. The therapeutic rationale remains the silicone film itself.
Best Silicone Cream for Raised Scars
Hypertrophic scars are raised, red, and confined to the boundaries of the original wound. They are among the scar types most commonly treated with silicone. Clinical goals include reducing scar height, improving pliability, and decreasing symptoms such as tightness or itching.
For older scars, a specialized old scar lightening serum may be discussed separately, but the evidence base for silicone remains focused mainly on raised scars rather than pigmentation alone. Some studies and reviews suggest that mature scars can still become softer or flatter with prolonged silicone use, though improvement is usually slower and less predictable than in newer scars.
Silicone Gel vs. Silicone Sheets
The choice between silicone gel and silicone sheets often comes down to patient compliance and the anatomical location of the scar.
| Feature | Silicone Gel | Silicone Sheets |
|---|---|---|
| Best For | Face, joints, irregular surfaces | Flat surfaces, under clothing |
| Visibility | Nearly invisible once dry | Visible (often beige or clear) |
| Compliance | High (easy to apply) | Moderate (can peel or itch) |
| Durability | Needs reapplication twice daily | Can be washed and reused for days |
| Occlusion Level | Moderate | High |
Silicone sheets provide a higher level of occlusion and are often preferred for surgical incisions on the chest, abdomen, or limbs where clothing can help hold them in place. However, on joints or the face, sheets frequently peel off due to movement or oils. In these cases, a self-drying gel is the more practical "best" option.
Research has shown that there is no significant difference in clinical efficacy between the two formats, provided they are used consistently. The "best" format is ultimately the one you will actually wear for the required 12 to 24 hours a day.
Evidence-Led Protocols for Post-Surgical Scar Management
Timing is everything in scar management. You should never apply silicone to an open wound. The general clinical consensus is to begin application as soon as the wound has "epithelialized" — meaning the skin has closed, there is no more oozing or crusting, and sutures have been removed.
Knowing when to apply scar cream after stitches is crucial. Typically, this occurs 10 to 14 days post-surgery. Once cleared by a surgeon, the following protocol is generally recommended:
- Cleanse: Gently wash the area with mild, fragrance-free soap and pat dry.
- Apply: Spread a very thin layer of silicone gel over the scar. A common mistake is applying too much; a thin film is all that is required to create the hydrated barrier.
- Duration: Aim for at least 12 hours of contact per day, though 24-hour coverage (reapplying morning and night) is optimal.
- Consistency: Continue the regimen for 60 to 90 days. For keloid-prone individuals or larger surgical scars, 6 months of use may be necessary.
Some practitioners also recommend gentle scar massage once the wound is fully closed. This can help break up dense collagen bundles, though the silicone barrier remains the primary therapeutic intervention.
Limitations and Contraindications of Topical Silicone Therapy
While medical-grade silicone is generally considered safe and chemically inert, it is not appropriate in every situation.
- Open wounds: Silicone should not be applied to skin that has not fully epithelialized. Using an occlusive product too early may irritate healing tissue and can trap moisture or contaminants against the wound.
- Active acne or folliculitis: Occlusive application over inflamed lesions may worsen irritation in some people, particularly on oily skin.
- Skin irritation: Although true allergy to silicone itself appears uncommon, irritant dermatitis, sweating, itching, or adhesive-related reactions can occur, especially with sheets.
- Pediatric use: Silicone is commonly used in children under medical guidance, but sheeting requires supervision in very young children because of detachment and choking concerns.
- Scar type limitations: Silicone is most often used for hypertrophic and keloid-prone scars. It is generally less useful for atrophic or sunken scars, such as many acne scars, because those scars reflect tissue loss rather than excess collagen deposition.
Safety reviews and clinical guidance generally support topical silicone as low risk when used on closed skin. A review indexed on PubMed also describes topical silicone gel as a commonly used and generally well-tolerated scar therapy. Even so, persistent redness, pain, drainage, or worsening inflammation should prompt clinical evaluation, as these findings may indicate infection, contact dermatitis, or another problem unrelated to normal scar maturation.
In addition, silicone is not a primary treatment for post-inflammatory hyperpigmentation. Although it may indirectly improve scar appearance by supporting better healing conditions, dedicated sun protection remains more important for preventing darkening of a healing scar.
Frequently Asked Questions about Silicone Scar Management
How long does it take to see visible results from silicone application?
Clinical studies show that while some softening may occur within 4 weeks, significant visible changes in height and redness typically require 2 to 3 months of consistent use. For mature scars, results may take up to 6 months to manifest.
Can silicone gels be used concurrently with makeup or sunscreen?
Yes. Once a self-drying silicone gel has completely set (usually 2–5 minutes), you can apply sunscreen or cosmetics over the film. This makes it an ideal choice for facial scars.
Is medical-grade silicone effective for older, mature scars?
Yes, though expectations should be managed. While silicone is most effective on "immature" scars (those less than 1 year old that are still red or purple), research has shown it can still improve the pliability and texture of older, white scars by restoring hydration to the dormant tissue.
Conclusion
The current clinical consensus is that medical-grade silicone is among the most widely recommended non-invasive options for the management of hypertrophic and keloid-prone scars. Evidence suggests that it may improve hydration, support a more favorable skin barrier environment, and help reduce scar thickness, stiffness, and color irregularity over time.
The key practical point is that results depend on sustained use and realistic expectations. Silicone does not remove scars completely, and study quality in this field is mixed. Still, dermatology reviews, clinical practice, and guideline-based care continue to support it as a reasonable first-line topical approach for many closed, raised scars.
For readers unsure what type of scar they have, a professional scar assessment can help determine whether silicone is likely to be useful and whether additional evaluation is needed.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Berman, B., Perez, O. A., Konda, S., et al. (2007). A review of the biologic effects, clinical efficacy, and safety of silicone elastomer sheeting for hypertrophic and keloid scar treatment and management. Dermatologic Surgery, 33(11), 1291–1303. https://pubmed.ncbi.nlm.nih.gov/17958580/
- Hsu, K. C., et al. (2017). Review of Silicone Gel Sheeting and Silicone Gel for the Prevention of Hypertrophic Scars and Keloids. Wounds, 29(5), 154–158. https://pubmed.ncbi.nlm.nih.gov/28570253/
- Puri, N., & Talwar, A. (2009). The efficacy of silicone gel for the treatment of hypertrophic scars and keloids. Journal of Cutaneous and Aesthetic Surgery, 2(2), 104–106. https://pmc.ncbi.nlm.nih.gov/articles/PMC2918339/
- Ahn, S. T., Monafo, W. W., & Mustoe, T. A. (1989). Topical silicone gel: a new treatment for hypertrophic scars. Surgery, 106(4), 781–786. https://pubmed.ncbi.nlm.nih.gov/2529659/
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/