The Waiting Game: When to Kickstart Your Post-Op Scar Routine
Timing your post-surgical scar care matters. Learn evidence-based protocols for when to start treatment after surgery and how to optimize healing at every stage of recovery.
When to Start Scar Treatment After Surgery
When to start scar treatment after surgery is one of the most common questions asked during surgical recovery — and the timing genuinely matters for long-term outcomes.
The short answer, supported by clinical evidence:
| Treatment Modality | Recommended Start Time |
|---|---|
| Petroleum jelly / wound ointment | Immediately post-surgery (day 0) |
| Gentle topical silicone gel | ~2 weeks post-surgery (once wound is fully closed) |
| Silicone sheeting | Day 0 to 2-4 weeks post-surgery |
| Scar massage | 2-3 weeks post-surgery |
| Topical scar creams | 2-4 weeks post-surgery |
| Sunscreen (SPF 30+) | ~3 weeks post-surgery, for 12-18 months |
| Laser therapy / dermabrasion | 2-3 months post-surgery |
| Surgical scar revision | 12-18+ months post-surgery |
The single most important rule: never apply scar treatment products to an open wound. The wound must be fully closed before any topical scar therapy begins.
Timing is not arbitrary. The skin heals in distinct biological phases — inflammation, proliferation, and remodeling — and each phase responds differently to intervention. Starting too early can disrupt the wound environment and delay healing. Starting too late may reduce how effectively treatment can influence collagen organization and scar texture.
Most people can begin a meaningful at-home scar care routine within two to four weeks of surgery, once the incision has fully closed and any sutures or scabs are gone. More advanced clinical treatments require the tissue to be considerably more mature.
The sections below explain the biology behind these timelines, what the research says about each treatment modality, and how to structure a post-operative scar routine that aligns with how skin actually heals.
Simple when to start scar treatment after surgery word guide:
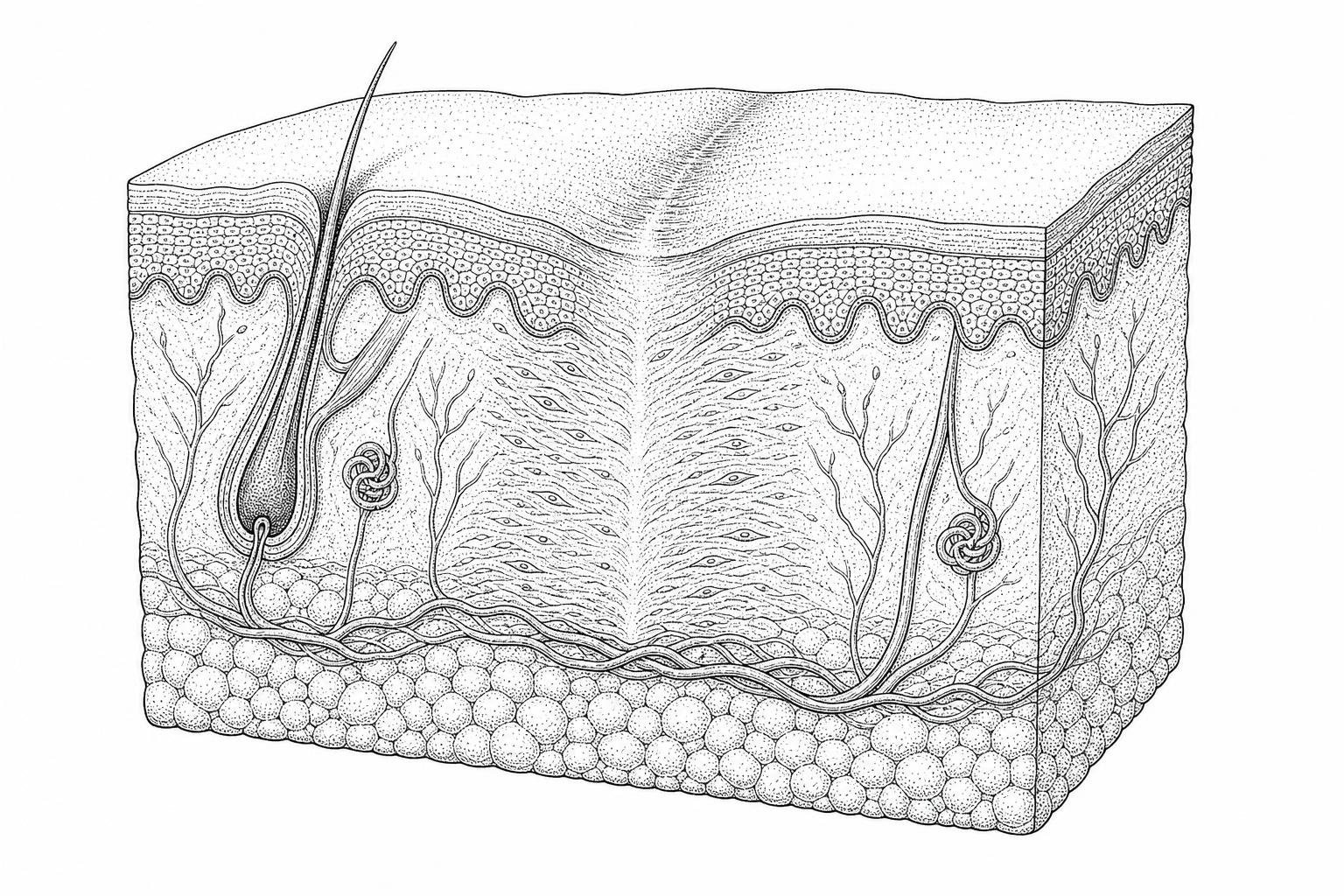
Biological Phases of Wound Repair and Tissue Regeneration
To understand when to start scar treatment after surgery, one must first understand the biological sequence of events that occurs after a surgical incision. Wound healing is a complex, overlapping process traditionally divided into four distinct phases: hemostasis, inflammation, proliferation, and remodeling.
Hemostasis and Inflammation (Days 1–5)
Immediately following surgery, the body initiates hemostasis to stop bleeding through platelet aggregation and the formation of a fibrin-platelet plug. This is followed closely by the inflammatory phase (typically days 1 to 5). During this time, neutrophils and macrophages migrate to the site to clear debris and bacteria. Clinical observations indicate that excessive or prolonged inflammation can lead to more significant scarring later, making early wound care—such as keeping the area clean and moist—critical.
Proliferation Phase (Days 5–21)
During the proliferation phase, the body focuses on "filling" the wound. Key cellular actors called fibroblasts migrate to the site to begin collagen synthesis. This stage involves angiogenesis (the formation of new blood vessels) and re-epithelialization, where new skin cells crawl across the wound surface at a rate of approximately 0.5 to 1 mm per day. Research published in Nature (Gurtner et al., 2008) highlights that the extracellular matrix (ECM) is rapidly constructed during this window, providing the structural framework for the developing scar.
Remodeling Phase (Day 21 to 1 Year+)
The final stage, remodeling or maturation, begins around the third week and can last for 12 to 18 months. During this phase, the chaotic "Type III" collagen produced during proliferation is gradually replaced by more organized "Type I" collagen. The scar’s tensile strength increases during this time, reaching about 50% of original skin strength by six weeks and peaking at approximately 80% by three months. Because the collagen is still being rearranged, this is the most effective window for interventions like silicone therapy and massage.

When to Start Topical and Pressure Therapies
The transition from "wound care" to "scar treatment" occurs at a specific clinical milestone: complete re-epithelialization. This means the wound is fully closed, no longer weeping, and the surgical scabs have detached naturally.
Key Milestones for Starting Treatment
For most post-operative patients, this milestone is reached between 2 and 4 weeks post-surgery. However, several factors influence this individual timeline:
- Suture Removal: Topical treatments (other than basic ointments like petroleum jelly) should generally wait until after sutures are removed or have fully dissolved.
- Scab Detachment: Forcing a scab to peel early can re-open the wound and trigger a new inflammatory cycle. One should wait until the skin is smooth and intact.
- Wound Closure: The "epithelial bridge" must be strong enough to withstand the mechanical stress of applying creams or massage.
Clinical guidelines emphasize that starting "active" treatments—such as silicone sheets or massage—too early can lead to wound dehiscence (the wound pulling apart) or infection. Conversely, waiting longer than six months to begin treatment may miss the "critical window" where collagen is most pliable and responsive to remodeling.
Comparing Treatment Start Times by Modality
Evidence-based protocols, such as those detailed in the post-surgery scar care guide, suggest the following chronological approach:
| Stage of Healing | Appropriate Intervention | Goal |
|---|---|---|
| Immediate (Day 0-14) | Petroleum jelly, antibiotic ointment | Maintain moisture, prevent crusting |
| Early Closed (Day 14-21) | Silicone gel, gentle scar cream after stitches | Regulate hydration, soothe itching |
| Active Remodeling (Week 3-8) | Silicone sheeting, scar massage | Flatten tissue, align collagen |
| Maturation (Month 3+) | Laser therapy, sun protection | Reduce redness, prevent darkening |
Clinical Guidelines for Initiating Specific Modalities
Different treatments work through different mechanisms. While some focus on hydration, others focus on mechanical tension or vascularity.
Protocol for Silicone-Based Occlusive Therapy
Silicone is considered the gold standard for non-invasive scar management. It works by creating an occlusive barrier that mimics the skin's natural stratum corneum. This reduces transepidermal water loss (TEWL), which signals the fibroblasts to slow down collagen production, preventing hypertrophic (raised) scars.
Research suggests that silicone gel can be introduced as soon as the wound is dry and closed (often day 10–14), while silicone sheeting, which may exert more "pull" on the skin, is often started at the 2-to-4-week mark. For optimal efficacy, clinical consensus suggests wearing silicone sheets for at least 12 hours a day for a duration of 3 to 6 months.
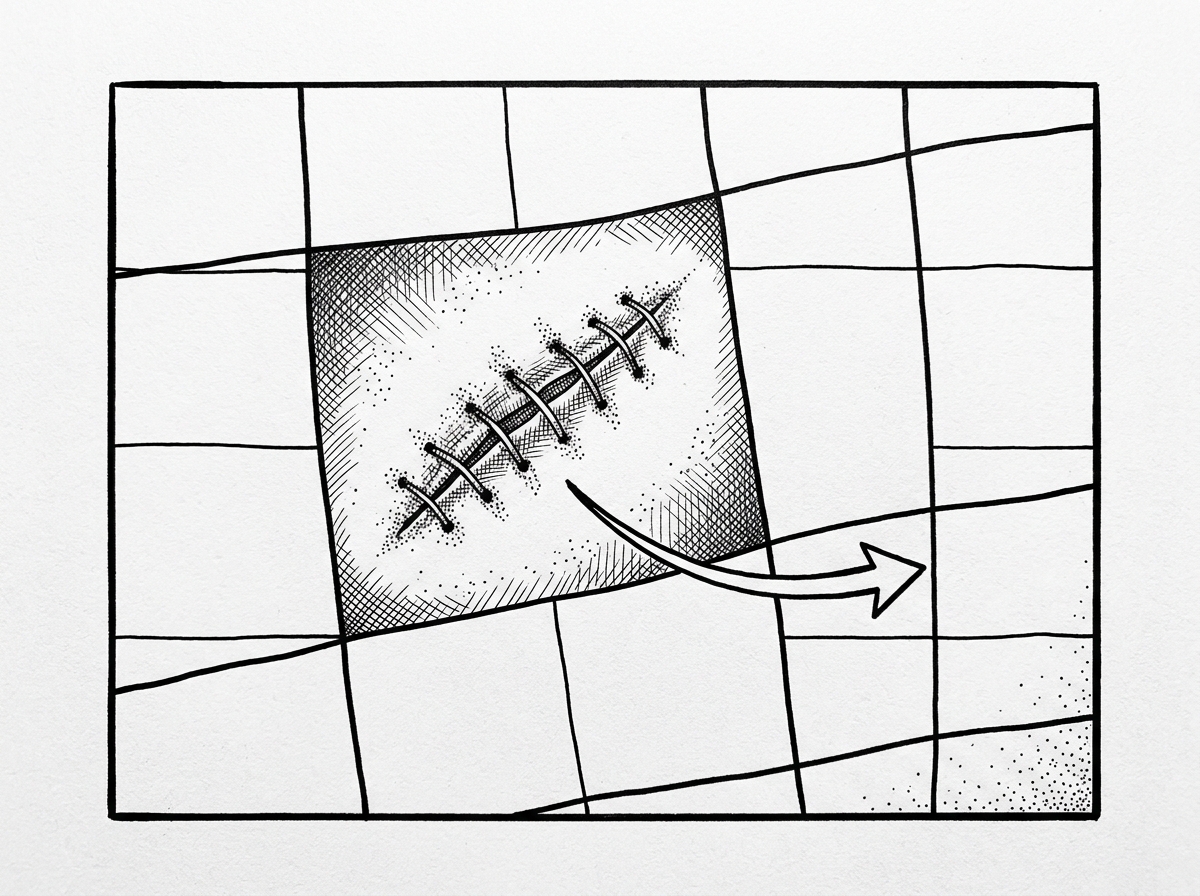
Temporal Guidelines for Manual Scar Mobilization
Massage therapy addresses the mechanical aspects of scar formation. By applying controlled pressure, massage helps break up fibrous adhesions and encourages collagen fibers to align in a more organized, "basket-weave" pattern rather than a tangled mass.
According to a review in Seminars in Plastic Surgery (Khansa et al., 2016), scar tissue massage therapy should typically begin 3 weeks post-surgery. The technique involves using the fingertips to apply firm, circular, or cross-friction pressure for about 10 minutes, twice daily. If the scar feels particularly rigid, a hard scar softening massage can be performed with a lubricant to improve tissue pliability.
Timing for Advanced Clinical Interventions
In cases where at-home treatments are insufficient, or for patients prone to abnormal scarring, advanced clinical interventions may be necessary. These are almost always delayed until the wound has reached a significant level of maturity.
Laser Therapy
Laser treatments, such as Pulsed Dye Laser (PDL) or Fractional CO2, target the vascularity and texture of the scar. PDL is often used to reduce the redness (erythema) of a scar by targeting hemoglobin in blood vessels. Evidence indicates that these treatments are typically most effective when performed 2 to 3 months post-surgery, as noted in clinical reviews on laser scar modulation. This allows the initial inflammatory redness to subside so the clinician can accurately target the persistent vascularity. For more detailed information, see the research on surgical scar laser treatment and laser treatment for surgical scars.
Dermabrasion and Revision
Dermabrasion, which physically "sands" the surface of the scar, is also generally performed in the 2-to-3-month window. However, surgical scar revision—where the old scar is excised and re-sutured—is rarely considered until at least 12 to 18 months have passed. This is because scars often improve significantly on their own during the full maturation cycle, and operating too early on immature tissue can lead to poor results.
Essential Precautions and Environmental Factors
Even the most rigorous scar routine can be undermined by environmental factors, particularly ultraviolet (UV) radiation.
The Role of Sun Protection
New scar tissue is highly susceptible to "post-inflammatory hyperpigmentation." UV exposure can cause the scar to darken permanently, a process that is difficult to reverse. Clinical guidelines recommend applying a broad-spectrum sunscreen with an SPF of 30 or higher starting roughly 3 weeks post-surgery. This should be continued for 12 to 18 months. Physical barriers, such as UV-protective clothing or silicone tape, provide even more reliable protection than creams alone.
Activities and Signs to Avoid
During the first 6 to 8 weeks of remodeling, it is vital to avoid:
- Mechanical Stress: Strenuous lifting or stretching that puts tension on the incision line, which can widen the scar.
- Irritants: Applying "natural" remedies like undiluted essential oils or Vitamin E oil too early, which have been shown in some studies to cause contact dermatitis in up to 30% of users without providing superior results to petroleum jelly.
- Picking: Disrupting the healing surface can introduce bacteria and lead to infection.
Warning Signs: Consult a healthcare professional if you notice increasing redness, warmth, swelling, pus (exudate), or if the wound begins to pull apart (dehiscence).
Clinical Inquiries and Patient Management Considerations
Can treatment begin while sutures are still in place?
Generally, no. Active scar treatments like silicone sheets or scar reduction creams should not be used while sutures are in place. The presence of sutures means the wound is still in the "proliferative" phase and is not yet fully sealed. The only exception is the application of plain petroleum jelly or a surgeon-approved antibiotic ointment to keep the site moist.
How long should a post-operative routine be maintained?
Consistency is the most significant factor in scar outcomes. Because the remodeling phase of collagen lasts up to a year, most clinical protocols suggest continuing silicone therapy and massage for at least 3 to 6 months. For those with a history of keloids or hypertrophic scars, a routine may need to be maintained for 12 months or longer to ensure the tissue remains stable.
What are the risks of starting treatment too early?
Starting too early—specifically before the wound is closed—carries several risks:
- Infection: Introducing creams or gels into an open wound can trap bacteria.
- Maceration: Over-hydrating an open wound with silicone can cause the tissue to become soggy and "macerated," which prevents proper closure.
- Contact Dermatitis: The fragile, newly forming skin may react poorly to the active ingredients in scar creams.
Summary of Clinical Recommendations
Determining when to start scar treatment after surgery is a balance between biological patience and proactive care. While the urge to treat a scar immediately is understandable, the most effective results come from following the body's natural healing timeline. Start with simple moisture (petroleum jelly) on day zero, transition to silicone and massage once the wound is dry and closed (weeks 2–4), and reserve advanced clinical interventions for the 3-month mark.
Every person's skin responds differently based on genetics, age, and the type of surgery performed. For a personalized approach, consider a formal scar assessment and always follow the specific post-operative instructions provided by your surgical team.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Gurtner, G. C., Werner, S., Barrandon, Y., & Longaker, M. T. (2008). Wound repair and regeneration. Nature, 453(7193), 314–321. https://pubmed.ncbi.nlm.nih.gov/18480812/
- Monstrey, S., et al. (2014). Updated scar management practical guidelines: non-invasive and invasive measures. Journal of Plastic, Reconstructive & Aesthetic Surgery, 67(8), 1017–1025. https://pubmed.ncbi.nlm.nih.gov/24888226/
- Khansa, I., Harrison, B., & Janis, J. E. (2016). Evidence-Based Scar Management: How to Improve Results with Technique and Technology. Plastic and Reconstructive Surgery, 138(3 Suppl), 165S–178S. https://pubmed.ncbi.nlm.nih.gov/27556757/