Retinoid vs Adapalene: Which Gel Wins the War on Acne Scars?
Retinoids and adapalene both target acne scars, but they work differently. Discover what the clinical evidence says about choosing the right topical retinoid for scar improvement.
Does Retinoid Cream Work for Scars
Retinoid cream for scars is one of the most clinically studied topical treatments available for improving scar appearance — particularly for atrophic acne scars and post-inflammatory hyperpigmentation (PIH).
For those looking for a quick orientation before diving deeper:
| Scar Type | Retinoid Efficacy | Typical Timeline |
|---|---|---|
| Post-inflammatory hyperpigmentation (PIH) | Strong evidence | 8-24 weeks |
| Atrophic acne scars (rolling, boxcar) | Moderate-strong evidence | 3-6 months |
| Surgical / post-stitch scars | Emerging evidence | 6-12 months |
| Hypertrophic or keloid scars | Limited evidence | Not first-line |
| Severe ice-pick scars | Weak evidence | Often requires procedural intervention |
The core mechanism is well established. Vitamin A derivatives — including retinol, retinaldehyde, and prescription-strength retinoic acid — accelerate cellular turnover, stimulate fibroblast activity, and increase collagen synthesis in the dermis. This directly addresses two of the main drivers of visible scarring: collagen loss and uneven pigmentation.
A 2015 retrospective clinical study published in Clinical, Cosmetic and Investigational Dermatology found that a combination of 0.025% retinoic acid and 12% glycolic acid produced measurable scar improvement in 91.4% of 35 patients after just 12 weeks. A separate randomized controlled trial published in JAMA Dermatology (2019) found that topical tazarotene gel (0.1%) produced scar severity improvements comparable to microneedling at six months — a notable finding for a home-based, non-invasive treatment.
These are not miracle results. Outcomes vary by scar type, skin tone, retinoid concentration, and consistency of use. Realistic expectations matter.
This article reviews the clinical evidence behind different retinoid formulations — including adapalene, tretinoin, and tazarotene — compares their mechanisms and tolerability profiles, and outlines evidence-based protocols for safe, effective use.
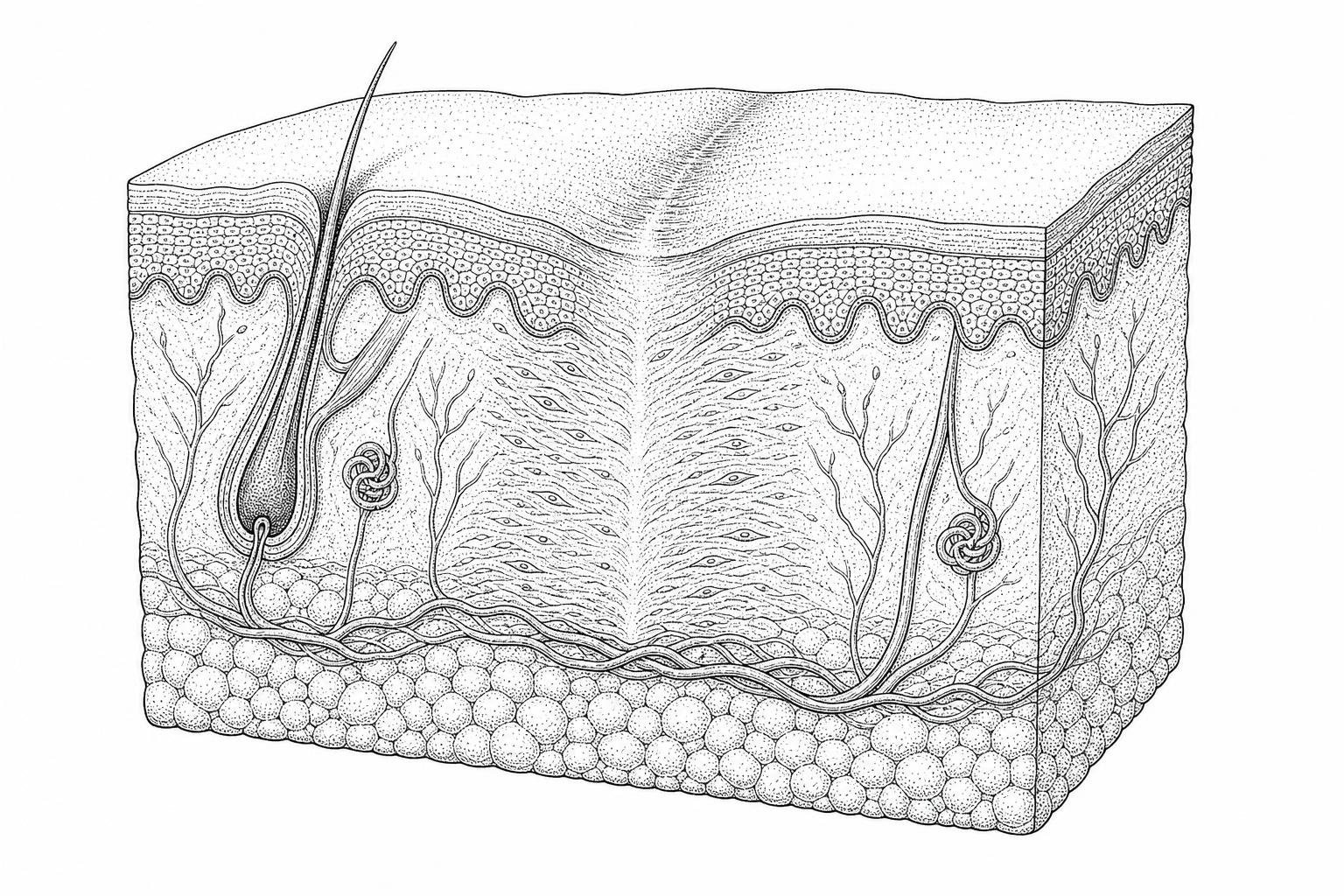
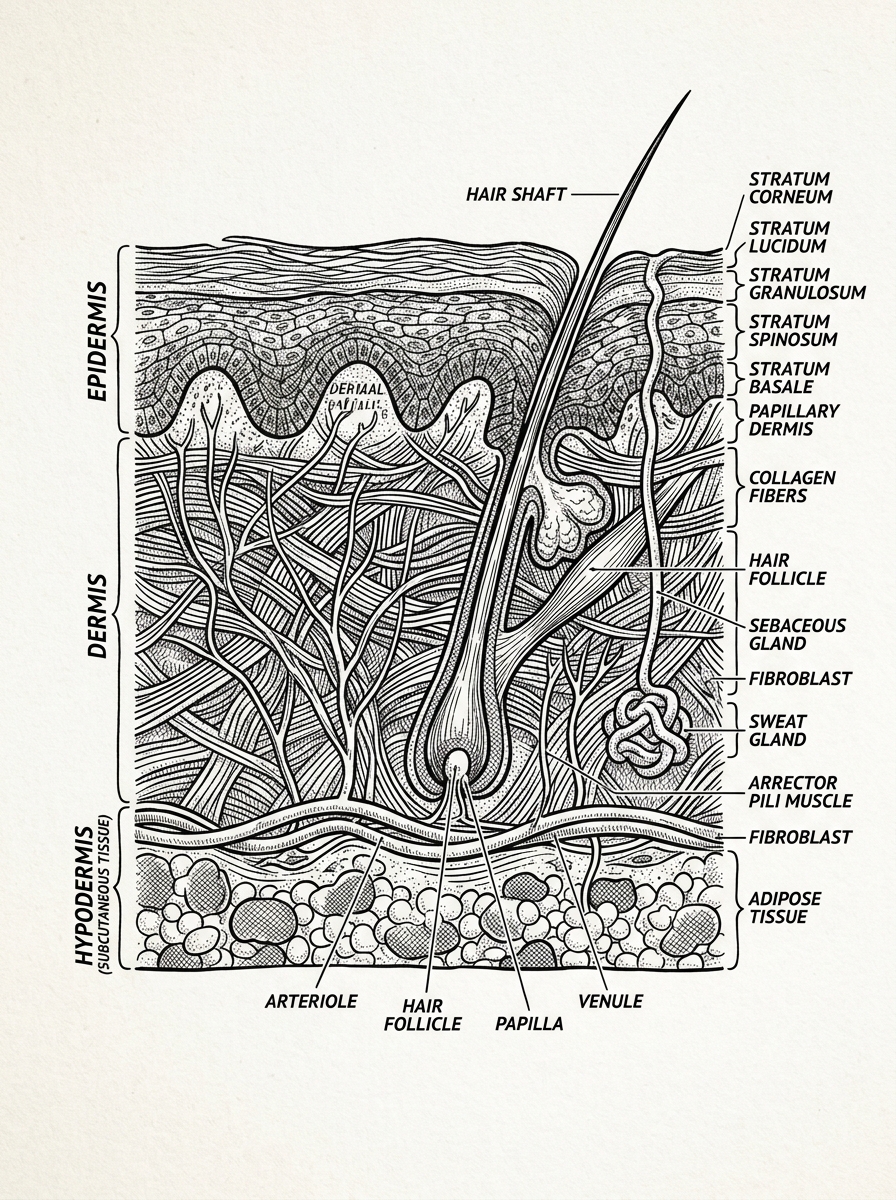
How Retinoids Help Skin Regenerate
To understand how a retinoid cream for scars functions, one must look at the cellular level of the skin. Retinoids are a family of compounds derived from Vitamin A that act as cell-signaling molecules. When applied topically, they bind to specific nuclear receptors—retinoic acid receptors (RAR) and retinoid X receptors (RXR)—within the skin cells.
How Retinoids Activate Collagen Rebuilding
The primary reason retinoids are effective for atrophic (pitted) scars is their ability to stimulate fibroblasts. Fibroblasts are the cells responsible for producing collagen and elastin, the structural proteins that give skin its "bounce" and thickness. Scientific research on retinoid mechanisms indicates that retinoids, particularly retinoic acid, can increase the production of Type 1 and Type 3 collagen by up to 80% over extended periods of use.
Furthermore, retinoids inhibit the activity of matrix metalloproteinases (MMPs). MMPs are enzymes that break down collagen. In the context of acne or injury, an overabundance of MMPs can lead to the destruction of the dermal matrix, resulting in the sunken appearance of atrophic scars. By suppressing these enzymes, retinoids help preserve existing collagen while fostering the growth of new tissue.
Accelerating the 28-Day Cycle
The human skin typically undergoes a renewal cycle every 28 days, where new cells are born in the deepest layer of the epidermis and eventually shed at the surface. Retinoids accelerate this process significantly. Clinical data suggests that consistent use of a potent retinoid cream for scars can reduce this cycle to 14–21 days. This rapid turnover forces the skin to shed damaged, pigmented cells more quickly and replace them with organized, healthy keratinocytes.
Comparison of Vitamin A Derivatives
Not all retinoids are created equal. Their efficacy depends on how many "conversion steps" they require to become retinoic acid, the only form the skin can actually use.
| Compound | Conversion Steps | Potency | Irritation Potential |
|---|---|---|---|
| Retinyl Palmitate | 3 Steps | Low | Low |
| Retinol | 2 Steps | Moderate | Moderate |
| Retinaldehyde | 1 Step | High | Moderate-High |
| Retinoic Acid (Tretinoin) | 0 Steps | Very High | High |
| Adapalene / Tazarotene | 0 Steps (Synthetic) | Very High | Variable |
Quantitative Analysis of Retinoid Efficacy in Atrophic Scarring and Dyschromia
The use of retinoid cream for scars is backed by substantial quantitative data, particularly regarding acne-related damage. In a 2015 study, researchers evaluated the "RAGA" protocol—a combination of retinoic acid (0.025%) and glycolic acid (12%). The results were significant: 91.4% of participants showed a measurable reduction in scar severity according to the Goodman and Baron Global Scarring Grading System (GSGS).
Addressing Post-Inflammatory Hyperpigmentation (PIH)
Scars are often accompanied by dark or red spots left behind after the initial wound heals. This is known as post-inflammatory hyperpigmentation. The RAGA study showed that 85.71% of patients experienced an improvement in these pigmented macules. Retinoids work here by inhibiting melanin transfer and encouraging the rapid shedding of pigment-laden cells. For those searching for an old scar lightening serum, a retinoid-based approach is often the clinical gold standard.
Epidermal Thickening and Texture Refinement
While atrophic scars involve the dermis, the texture of the scar is determined by the epidermis. Chronic use of retinoids has been shown to increase epidermal thickness. This "plumping" effect can make shallow boxcar or rolling scars appear less prominent. When combined with the best scar reduction cream formulations, retinoids help smooth the overall "orange peel" texture often associated with long-term acne damage.
Optimizing Results with Retinoid Cream for Scars
Monotherapy (using only one active ingredient) is often less effective than combination therapy. Science suggests that pairing retinoids with specific ingredients can enhance their penetration and efficacy:
- Glycolic Acid: As an Alpha Hydroxy Acid (AHA), it thins the stratum corneum (the outermost layer of dead skin), allowing the retinoid to penetrate deeper into the dermis.
- Hyaluronic Acid: Retinoids can be drying. Hyaluronic acid helps maintain hydration levels, reducing the risk of inflammation which could otherwise worsen scarring.
- Niacinamide: This B-vitamin stabilizes the skin barrier and reduces the redness associated with "retinization," the adjustment period when starting a new treatment.
Safety Considerations for Retinoid Cream for Scars
The potency of retinoids comes with a "tax" on the skin barrier. Common side effects include:
- Erythema (Redness): A sign of increased blood flow and initial irritation.
- Xerosis (Dryness): Retinoids reduce the production of certain surface oils.
- Photosensitivity: Because retinoids thin the top layer of dead skin, the underlying fresh skin is highly susceptible to UV damage.
Proper post surgery scar care dictates that one should never apply a high-strength retinoid to an open wound or a fresh incision that has not fully epithelialized.
Comparative Pharmacology: Adapalene, Tretinoin, and Tazarotene in Atrophic Scar Remediation
When choosing a retinoid cream for scars, the specific molecule matters. Third-generation retinoids like adapalene and tazarotene were designed to be more "receptor-selective," meaning they target the pathways involved in cell growth and inflammation while ignoring some of the pathways that cause irritation.
The Tazarotene vs. Microneedling Study
One of the most compelling pieces of evidence for topical treatment appeared in JAMA Dermatology. A split-face study compared 0.1% tazarotene gel to professional microneedling sessions. After six months, both treatments showed nearly identical results in reducing quantitative scar severity. This suggests that for patients who cannot afford or tolerate procedural interventions, a high-potency retinoid may offer a viable alternative.
Receptor Selectivity and Potency
- Tretinoin (Retinoic Acid): The "all-rounder." It binds to all RAR receptors. It is highly effective but often the most irritating.
- Adapalene: Primarily targets RAR-beta and RAR-gamma. It is generally more stable and less irritating than tretinoin, making it a popular choice for those with sensitive skin.
- Tazarotene: Often considered the most potent of the three. It has a high affinity for RAR-gamma, which is the predominant receptor in the epidermis.
Knowing when to apply scar cream after stitches is vital; typically, one must wait until the wound is closed and the "remodeling phase" of healing has begun, which is usually several weeks post-injury.
Evidence-Based Clinical Protocols for Optimized Topical Retinoid Administration
To achieve the 75–85% success rates seen in clinical trials for pigment and texture improvement, the application method must be precise. The goal is to maximize "contact time" while minimizing "barrier disruption."
The "Low and Slow" Method
The skin needs time to upregulate its receptors to handle Vitamin A.
- Weeks 1-2: Apply the retinoid cream for scars once every three nights.
- Weeks 3-4: Increase to every other night if no significant peeling occurs.
- Month 2+: Gradually move toward nightly application.
The "Retinoid Sandwich" Technique
For those with reactive skin, clinicians often recommend the "sandwich" method:
- Apply a thin layer of moisturizer.
- Apply a pea-sized amount of retinoid.
- Apply a second layer of moisturizer. This buffers the penetration speed without negating the long-term benefits.
Supporting the Remodeling Phase
Scar maturation is a slow process. Collagen remodeling can continue for up to 12 months after an injury. Consistency is more important than frequency; missing a night is better than forcing an application on irritated, "burned" skin. Additionally, scar tissue massage therapy can be used in the mornings to help break up dense collagen fibers, while the retinoid works at night to reorganize them. For older, tougher scars, a hard scar softening massage may further improve the pliability of the tissue.
Therapeutic Limitations and Contraindications in Retinoid-Based Scar Therapy
While retinoid cream for scars is a powerful tool, it is not a panacea. There are specific scenarios where topical Vitamin A is either ineffective or dangerous.
Hypertrophic and Keloid Scars
Hypertrophic scars and keloids are characterized by an overproduction of collagen. Because retinoids stimulate collagen synthesis, they are generally not the first-line treatment for these raised scars. In some cases, very high-strength retinoids may help soften the texture, but most clinical guidelines prioritize silicone sheeting, pressure therapy, or corticosteroid injections.
Pregnancy and Breastfeeding
This is a critical safety boundary. Oral retinoids (like isotretinoin) are known teratogens, meaning they cause birth defects. While the systemic absorption of topical retinoids is low, the medical consensus—and the advice of organizations like the American Academy of Dermatology—is to avoid all retinoids during pregnancy and breastfeeding as a precautionary measure.
Severe Ice-Pick Scars
Ice-pick scars are narrow but deep, often extending into the deep dermis or subcutaneous fat. Topical creams, even prescription-strength retinoids, rarely have the "reach" to fill these deep columns. These usually require procedural interventions such as:
- TCA CROSS: Chemical reconstruction of skin scars.
- Punch Excision: Surgically removing the scar.
- Laser Resurfacing: Using fractional CO2 or Erbium lasers to vaporize the scar tissue.
Clinical Considerations and Common Inquiries Regarding Retinoid Therapy
How long does it take for retinoids to fade acne scars?
Visible changes in skin texture usually begin at the 4–6 week mark as cellular turnover increases. However, significant remodeling of atrophic scars and fading of deep PIH typically requires 3 to 6 months of consistent use.
Can retinoids be used on surgical or post-stitch scars?
Yes, but only after the wound has completely closed and the initial inflammatory phase has passed (usually 4–6 weeks). Retinoids can help the new collagen fibers organize in a more linear, "natural" fashion, making the scar less noticeable.
Is adapalene or tretinoin more effective for pitted scars?
Tretinoin (retinoic acid) has more historical data supporting its use for collagen induction. However, recent studies suggest that 0.1% or 0.3% adapalene is highly effective for atrophic scars with a lower risk of the "tretinoin purge" and irritation.
Summary of Therapeutic Outcomes and Clinical Recommendations
From the perspective of scar-healing.com, the evidence for retinoid cream for scars is robust but requires a disciplined approach. Whether one chooses over-the-counter retinol or prescription-strength tazarotene, the biological principles remain the same: accelerate turnover, boost collagen, and regulate pigment.
Topical retinoids represent a bridge between basic skincare and invasive procedures. For many, they provide a sufficient increase in skin quality to avoid the cost and downtime of lasers. However, for deep, structural scarring, they serve best as a "pre-treatment" to optimize the skin's health before professional intervention.
If you are unsure of your scar type or the best course of action, consider utilizing the Scar Healing assessment tool to better understand your skin's specific needs.
Works Cited
- Chandrashekar, B. S., Ashwini, K. R., Vasanth, V., & Navale, S. (2015). Retinoic acid and glycolic acid combination in the treatment of acne scars. Clinical, Cosmetic and Investigational Dermatology, 8, 281–288. https://pubmed.ncbi.nlm.nih.gov/25821727/
- Afra, T. P., et al. (2019). Topical Tazarotene Gel, 0.1%, as a Novel Treatment Approach for Atrophic Postacne Scars: A Randomized Active-Controlled Clinical Trial. JAMA Facial Plastic Surgery, 21(2), 87–95. https://pubmed.ncbi.nlm.nih.gov/30452511/
- Mukherjee, S., et al. (2006). Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clinical Interventions in Aging, 1(4), 327–348. https://pubmed.ncbi.nlm.nih.gov/18046911/
- Thielitz, A., Abdel-Naser, M. B., Gollnick, H. (2008). Topical retinoids in acne – an evidence-based overview. Journal der Deutschen Dermatologischen Gesellschaft, 6(12), 1023–1031. https://pubmed.ncbi.nlm.nih.gov/18397320/