What the Science Says: The Best Cream for Pimples and Dark Spots
Finding one cream that tackles both active pimples and lingering dark spots means targeting two different skin processes at once. Discover which clinically backed ingredients address both.
Why Finding the Best Cream for Pimples and Dark Spots Is Harder Than It Looks
The best cream for pimples and dark spots addresses two distinct biological processes simultaneously: active inflammatory acne lesions and post-inflammatory hyperpigmentation (PIH). These require different active ingredients, which is why single-ingredient products often fall short.
Quick answer — key ingredients to look for:
| Concern | Evidence-Based Ingredient | Typical OTC Strength |
|---|---|---|
| Active pimples | Benzoyl peroxide | 2.5% – 5% |
| Active pimples | Salicylic acid | 0.5% – 2% |
| Active pimples | Adapalene | 0.1% |
| Dark spots / PIH | Niacinamide | 5% – 10% |
| Dark spots / PIH | Azelaic acid | 10% |
| Dark spots / PIH | Tranexamic acid | 2% – 5% |
| Both concerns | Azelaic acid | 10% (OTC) |
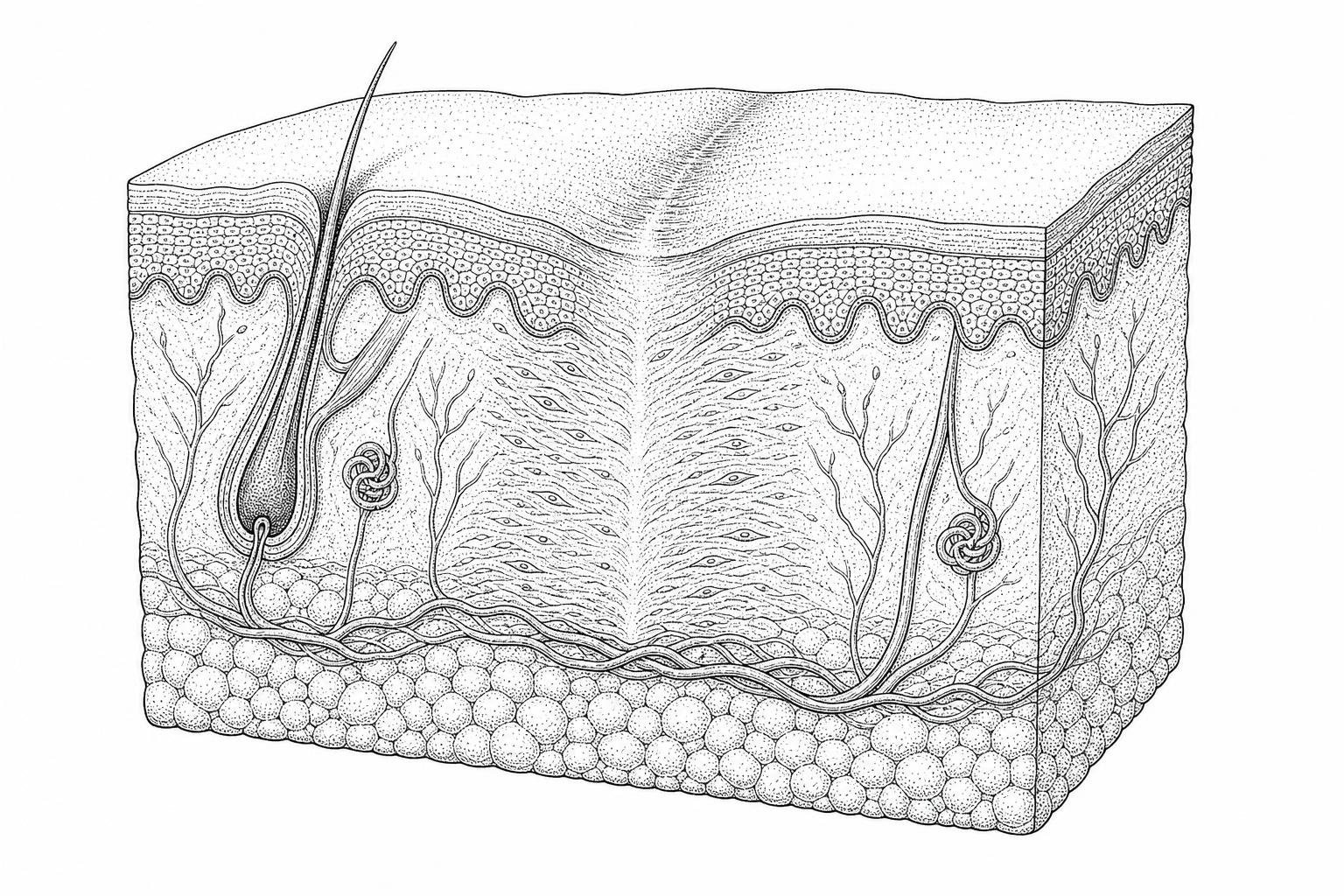
Most people dealing with acne already know the frustration: the pimple clears, and a dark mark takes its place. Clinically, this mark is called post-inflammatory hyperpigmentation — an excess of melanin (the pigment that gives skin its color) deposited in the dermis after the skin's inflammatory response settles down.
Acne itself begins in the sebaceous glands — oil-producing structures attached to hair follicles. When excess sebum, dead skin cells, and Cutibacterium acnes bacteria combine, they trigger an inflammatory cascade. The skin's attempt to heal that inflammation is what leaves the dark spot behind.
According to Mayo Clinic, it may take 2 to 3 months of consistent daily use before over-the-counter topical treatments produce visible results — a realistic expectation that many product labels understate.
The sections below review the clinical evidence behind the most studied topical agents, how they work on a biological level, and how to build a routine that addresses both concerns without compromising the skin barrier.
Clinical Criteria for Selecting the Best Cream for Pimples and Dark Spots
When evaluating a topical treatment, clinical efficacy depends on more than just the active ingredient. Factors such as the vehicle (cream vs. gel), the concentration of the molecule, and the ability of the formula to penetrate the stratum corneum (the outermost layer of skin) determine whether a product will resolve a blemish or simply sit on the surface.
Dermal penetration is a significant hurdle in acne therapy. Because acne occurs within the hair follicle and sebaceous gland, the best cream for pimples and dark spots must be formulated to bypass the skin's lipid barrier. Some modern formulations use micronized particles or liposomal delivery systems to ensure the active agents reach the target site.
Furthermore, the term "non-comedogenic" is a critical clinical baseline. This indicates that the product has been tested and found unlikely to block pores, which would otherwise exacerbate the very condition the cream is intended to treat.
For more detailed information on selecting products, see this Scientific research on nonprescription acne treatments.
Identifying the Best Cream for Pimples and Dark Spots Based on Skin Type
- Oily Skin: Individuals with high sebum production often benefit from gel-based or "matte-finish" creams. These formulations typically exclude heavy oils and may include starches or clays to absorb excess surface lipids.
- Sensitive Skin: Those prone to erythema (redness) or stinging should prioritize lower concentrations of active ingredients. For example, a 2.5% benzoyl peroxide cream is often better tolerated than a 10% version while providing comparable results.
- Combination Skin: This skin type requires a "zonal" approach. A powerful spot treatment may be used on the oily T-zone, while a more hydrating, barrier-supportive cream is applied to the drier cheeks.
- Melanin-Rich Skin: Patients with darker skin tones are more susceptible to post-inflammatory hyperpigmentation. In these cases, it is vital to avoid over-exfoliation, which can trigger further pigment production. Ingredients like azelaic acid are particularly effective here as they target abnormal melanocytes.
How to pick a cream that stays effective
Topical agents are often chemically unstable. Vitamin C (ascorbic acid) and retinoids are notoriously sensitive to light and oxygen. When these ingredients oxidize, they lose their biological potency and may even cause skin irritation.
Clinical preference is often given to airless pumps or opaque tubes rather than jars. Jars expose the cream to air and potential bacterial contamination from fingertips every time they are opened. Additionally, the pH of the formulation must be precisely balanced; for instance, salicylic acid requires an acidic environment (usually a pH of 3 to 4) to effectively exfoliate the pore lining.

Mechanisms of Action: How Topical Agents Resolve Inflammatory Lesions
To treat a pimple, a cream must address one of the four pillars of acne formation: follicular hyperkeratinization (clogged pores), excess sebum, bacterial growth, or inflammation.
Benzoyl peroxide and salicylic acid remain the "gold standards" for over-the-counter care. More recently, the introduction of topical retinoids like adapalene and hormonal modulators like clascoterone has expanded the clinical toolkit. These agents work by normalizing how skin cells are shed and reducing the inflammatory signals sent by the immune system.
For deeper insights into how these medications function, refer to this Scientific research on acne medication mechanisms. If you are looking for ways to reduce acne scars fast, understanding these mechanisms is the first step toward prevention.
The Role of 2% Salicylic Acid in Pore Desquamation
Salicylic acid is a Beta Hydroxy Acid (BHA). Unlike Alpha Hydroxy Acids (AHAs), which are water-soluble, salicylic acid is oil-soluble. This allows it to penetrate deep into the pore to dissolve the "glue" (lipids) holding dead skin cells together.
By promoting desquamation (the shedding of the skin's top layer), salicylic acid prevents the formation of comedones (blackheads and whiteheads). Clinical observations show that consistent use of a 2% concentration can significantly reduce the number of non-inflammatory lesions over a six-week period.
Benzoyl Peroxide Efficacy: 2.5% vs. 10% Preparations
Benzoyl peroxide is a potent antimicrobial agent that introduces oxygen into the pore. Because C. acnes bacteria are anaerobic (they cannot survive in the presence of oxygen), benzoyl peroxide kills them directly without the risk of antibiotic resistance.
A common misconception is that a higher percentage is always better. However, clinical studies have demonstrated that 2.5% benzoyl peroxide is just as effective as 10% preparations for treating mild to moderate acne, but with significantly less dryness, peeling, and irritation. The lower strength is often considered the best cream for pimples and dark spots for those starting a new regimen.
Best ingredients for dark spots after breakouts
Once the inflammatory phase of a pimple subsides, the focus shifts to resolving the "dots" left behind. This requires ingredients that can inhibit tyrosinase—the enzyme responsible for melanin production—or prevent the transfer of pigment to the skin's surface.
Research indicates that combining multiple brightening agents is more effective than using one in isolation. You can explore more about dark scar removal methods to understand how these ingredients fit into a broader dermatological context.
Niacinamide at 10% Concentration for Barrier Repair
Niacinamide, or Vitamin B3, is a multitasking molecule. At a 10% concentration, evidence suggests it can inhibit the transfer of melanosomes (pigment granules) from melanocytes to keratinocytes. Beyond its brightening effects, niacinamide stimulates the production of ceramides, which are essential lipids that keep the skin barrier intact. This makes it an excellent choice for those who experience dryness from traditional acne medications.
Azelaic Acid for Dual-Action Treatment
Azelaic acid is a naturally occurring dicarboxylic acid. It is unique because it treats both active acne and dark spots. It possesses antimicrobial properties similar to benzoyl peroxide but also acts as a selective tyrosinase inhibitor. It specifically targets hyperactive melanocytes (the ones producing too much pigment) while leaving normal skin cells alone.
While 15-20% concentrations require a prescription, 10% over-the-counter formulations have shown significant success in clinical trials for reducing both lesion count and the intensity of post-acne marks.
Retinoids vs. hydroxy acids for scarring
Retinoids, derived from Vitamin A, are considered the cornerstone of acne therapy. They communicate with skin cells to speed up turnover and stimulate collagen production. This process not only clears current pimples but also helps remodel the tissue to prevent the formation of "pitted" or atrophic scars.
Hydroxy acids (like glycolic or lactic acid) work more superficially by dissolving the bonds between surface cells. While effective for texture, they do not offer the same deep-level remodeling as retinoids. For those dealing with more permanent changes in skin texture, a microneedling for keloid scars guide may offer additional insights.
Adapalene 0.1% as a First-Line Retinoid
Adapalene was the first prescription-strength retinoid to become available over-the-counter in the United States. It is "receptor-selective," meaning it targets specific retinoic acid receptors in the skin that regulate inflammation and cell turnover. This selectivity typically results in better tolerability compared to older retinoids like tretinoin. It is a primary recommendation for inflammatory acne and preventing the initial stages of scarring.
Tazarotene for Severe Lesions and Remodeling
Tazarotene is a third-generation retinoid, usually available by prescription. It binds to a different set of receptors than adapalene and is often used for more severe cases of acne. Interestingly, a small clinical study found that a 0.1% tazarotene gel was nearly as effective as multiple sessions of microneedling for improving the appearance of indented acne scars. It is a powerful tool for tissue remodeling but requires careful medical supervision due to its high potency.
Building a routine that works
Applying the best cream for pimples and dark spots is only half the battle; the rest of the routine must support the skin's health.
- Cleansing: Use a mild, pH-balanced cleanser twice daily. Avoid harsh scrubs, which can create micro-tears and worsen inflammation.
- Treatment: Apply acne or dark spot creams to clean, dry skin.
- Moisturizing: Even oily skin needs hydration. Look for oil-free, non-comedogenic moisturizers containing hyaluronic acid or glycerin.
- Protection: This is the most critical step. UV exposure darkens hyperpigmentation and can make acne marks permanent. A broad-spectrum SPF 30+ is mandatory when using retinoids or exfoliating acids.
Managing Side Effects: Peeling and Erythema
Most effective acne treatments cause an initial period of "purging" or irritation, often called retinoid dermatitis. To mitigate this, clinicians suggest the "sandwich method": applying a thin layer of moisturizer, then the treatment cream, followed by another layer of moisturizer. This buffers the active ingredients without neutralizing their efficacy.
Timeline for Visible Results in Skin Regeneration
Patience is a clinical requirement. Because the skin's natural turnover cycle takes approximately 28 to 30 days, and deep-seated pigment takes even longer to rise to the surface and shed, most patients will not see significant improvement for at least 8 to 12 weeks. Compliance—using the product every single day as directed—is the single greatest predictor of success.
Conclusion
Banishment of "spots and dots" is a marathon, not a sprint. By selecting the best cream for pimples and dark spots based on clinical evidence—prioritizing ingredients like adapalene, azelaic acid, and niacinamide—individuals can effectively manage both active breakouts and the lingering marks they leave behind.
For those dealing with older marks, a dedicated old scar lightening serum may be a necessary addition to the regimen. Always remember that while over-the-counter options are vast, persistent or severe acne warrants a consultation with a board-certified dermatologist.
For more resources on skin regeneration and healing, visit the Scar Healing homepage.
Frequently Asked Questions about Acne and Dark Spots
Can benzoyl peroxide and retinoids be used together?
Historically, benzoyl peroxide was known to deactivate certain retinoids like tretinoin. However, modern formulations, especially those containing adapalene, are much more stable. Many dermatologists recommend using benzoyl peroxide in the morning and a retinoid at night to maximize efficacy while minimizing irritation.
How does sun exposure affect post-acne marks?
UV radiation stimulates melanocytes to produce more melanin. When a area of skin is already inflamed (like a healing pimple), the sun's rays act as a "stain," darkening the red or pink mark into a stubborn brown spot. Daily sunscreen use is the most effective way to ensure dark spots fade quickly.
Why does acne often worsen before improving with new treatments?
This is known as "purging." Ingredients like retinoids and salicylic acid speed up cell turnover, which can cause "pre-clogs" that were already deep in the pore to rise to the surface all at once. This phase typically lasts 2 to 4 weeks and is a sign that the medication is working to clear the skin from the inside out.
Works Cited
- Zaenglein, A. L., et al. (2016). Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology, 74(5), 945–973.e33. https://pubmed.ncbi.nlm.nih.gov/26897386/
- Davis, E. C., & Callender, V. D. (2010). Postinflammatory Hyperpigmentation: A Review. Journal of Clinical and Aesthetic Dermatology, 3(7), 20–31. https://pmc.ncbi.nlm.nih.gov/articles/PMC2921758/
- Castillo, D. E., & Keri, J. E. (2018). Chemical peels in the treatment of acne: patient selection and perspectives. Clinical, Cosmetic and Investigational Dermatology, 11, 365–372. https://pmc.ncbi.nlm.nih.gov/articles/PMC6053170/
- Fabbrocini, G., et al. (2010). Acne Scars: Pathogenesis, Classification and Treatment. Dermatology Research and Practice, 2010, 893080. https://pmc.ncbi.nlm.nih.gov/articles/PMC2958495/
- Mukherjee, S., et al. (2006). Retinoids in the treatment of skin aging: an overview. Clinical Interventions in Aging, 1(4), 327–348. https://pubmed.ncbi.nlm.nih.gov/18046911/