How to Say Goodbye to Stubborn Abdominal Keloids
Abdominal keloids are notoriously stubborn, but combination therapies — silicone, steroid injections, and surgery with adjuvant radiation — can achieve lasting reduction.
Treating Abdominal Keloid Scars
Abdomen keloid scar reduction refers to the clinical management of raised, fibrous overgrowths that extend beyond the original wound boundary on the abdominal skin. These are not ordinary scars. Keloids are a fibroproliferative disorder — meaning the body continues producing excess collagen long after a wound has closed, creating a lesion that can grow, harden, itch, and cause pain.
The abdomen is one of the most common sites for keloid formation. This is largely because the lower abdominal skin is under constant mechanical tension — from movement, breathing, and posture. Common triggers include C-section incisions, hernia repairs, laparoscopic port sites, and abdominoplasty procedures.
Quick-reference summary: abdomen keloid scar reduction options
| Treatment | Evidence Level | Typical Recurrence Rate |
|---|---|---|
| Silicone gel sheeting | Strong (first-line) | Significant improvement in up to 90% of cases |
| Corticosteroid injections | Strong (first-line) | 9–50% recurrence |
| Surgery alone | Strong | 45–100% recurrence |
| Surgery + radiotherapy | Strong | 0–8.6% recurrence |
| Cryotherapy | Moderate | Variable |
| Laser therapy | Moderate | Varies by type |
| PRP + surgery + radiation | Emerging | ~4.5% recurrence (short follow-up) |
The high recurrence rates after surgery alone make keloids particularly frustrating to manage. Clinical evidence consistently shows that combination therapies — such as surgical excision followed by radiation or corticosteroid injections — outperform any single treatment.
For those dealing with visible, persistent abdominal scarring that affects daily comfort or self-confidence, understanding the full range of evidence-based options is the first step. This guide covers the biology behind keloid formation, clinically supported reduction strategies, and what realistic outcomes look like — drawing on peer-reviewed research and established clinical guidelines.
For more on abdominal scar management broadly, see Abdominal Scars.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Why abdominal keloids form
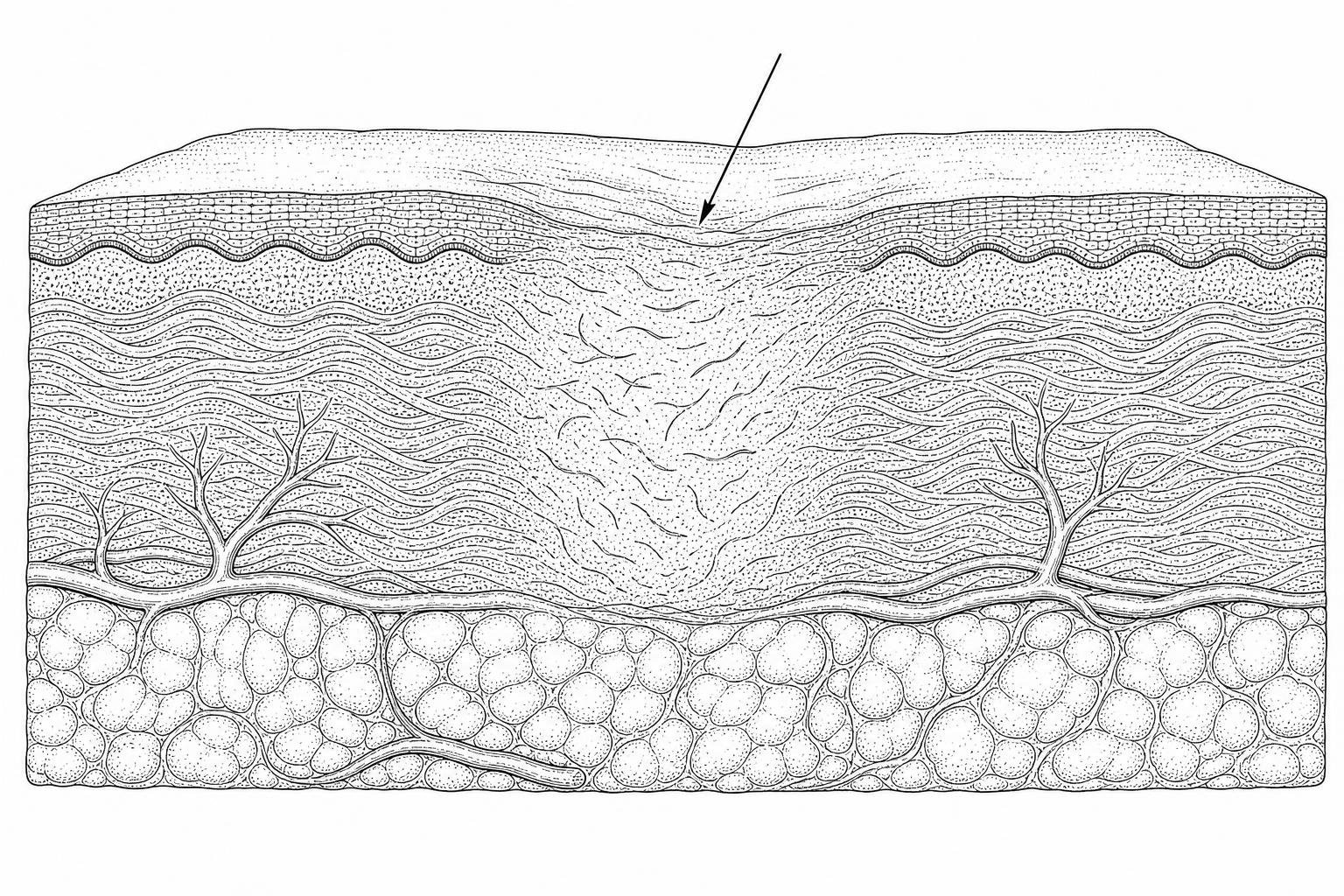
The formation of a keloid is fundamentally a failure in the body's wound-healing "off switch." Under normal circumstances, once a wound is closed, the production of collagen slows down and the scar matures. In keloid-prone individuals, fibroblasts—the cells responsible for synthesizing the structural framework of the skin—remain hyperactive. This leads to an excessive accumulation of extracellular matrix components, primarily types I and III collagen.
Research indicates that mechanical tension is a primary driver of this process. The lower abdomen and suprapubic regions are high-tension areas. As the skin stretches during daily activities, it triggers inflammatory pathways that signal fibroblasts to continue producing collagen. This chronic inflammation is why abdominal keloids often feel firm, tender, or itchy.
Distinguishing Keloids from Hypertrophic Scars on the Abdomen
It is clinically vital to distinguish between a keloid and a hypertrophic scar, as the treatment pathways differ significantly. While both are raised and can appear red or purple, their biological behavior is distinct:
- Boundaries: Hypertrophic scars remain within the original margins of the wound or incision. Keloids are "invasive," spreading into the surrounding healthy skin.
- Regression: Hypertrophic scars often flatten or fade over several years. Keloids rarely regress on their own and may continue to grow indefinitely.
- Histology: Under a microscope, hypertrophic scars show wavy, organized collagen patterns. Keloids exhibit thick, disorganized collagen bundles with no distinct orientation.
Misdiagnosing a keloid as a simple hypertrophic scar can lead to ineffective treatment. For instance, while a hypertrophic scar might respond well to a Hypertrophic Scar Reduction Cream, a true keloid usually requires more aggressive intervention.
Risk Factors for Developing Abdominal Keloids
While anyone can develop a keloid, certain populations are at a significantly higher risk. Clinical data suggests the following factors are most influential:
- Skin Pigmentation: Keloids are significantly more common in individuals with darker skin tones (Fitzpatrick scales IV-VI). Prevalence rates are estimated at up to 16% in certain African populations and approximately 10% in African-American communities.
- Age: Most keloids develop between the ages of 10 and 30. They are less common in the very young or the elderly.
- Genetics: A family history of keloid formation is a strong predictor. Some research suggests an autosomal dominant inheritance pattern with incomplete penetrance.
- Surgical Trauma: Abdominal surgeries, particularly C-sections and abdominoplasties, are major triggers. The combination of deep tissue trauma and high skin tension creates the "perfect storm" for keloid development.
For a deeper dive into the genetic and environmental triggers, refer to the clinical overview of Keloid Scars.
Treatment Plans for Abdominal Keloids
Management of abdominal keloids typically follows a stepped approach, starting with non-invasive methods before moving to medical or surgical interventions.

How Silicone Gel Performs Against Abdominal Keloids
Silicone gel and silicone gel sheeting are considered the "gold standard" for non-invasive abdomen keloid scar reduction. Although the exact mechanism is still being studied, evidence suggests that silicone works through occlusion and hydration. By trapping moisture, silicone reduces the activity of the capillaries and fibroblasts, effectively "calming" the scar tissue.
To see results, clinical guidelines recommend:
- Duration: Wearing the sheeting for 12 to 24 hours per day.
- Timeline: Consistent use for 3 to 6 months.
- Pressure: Combining silicone with pressure garments (applying 24–30 mmHg of pressure) can improve outcomes by further restricting blood flow to the overactive tissue.
Studies have shown that Silicone Gel for Scars can result in up to a 90% improvement in the texture and color of excessive scars.
Topical Agents and Emerging Non-Invasive Options
Beyond silicone, several topical treatments are used with varying degrees of success:
- Onion Extract: Some clinical studies suggest that onion extract (Allium cepa) can improve scar height and redness, though it is generally considered less effective than silicone.
- Imiquimod: Originally an antiviral/antitumor cream, applying 5% imiquimod after surgical excision may help modulate the immune response to prevent recurrence, though some studies report mixed results.
- Microneedling: This technique involves creating controlled micro-injuries to "reset" the healing process. When combined with topical steroids, Microneedling For Scars can help medications penetrate deeper into the dense keloid tissue.
Advanced Combination Therapies
When non-invasive methods fail, medical professionals often turn to intralesional treatments or surgery. However, the most critical takeaway from recent research is that surgery alone is rarely enough.
| Treatment Strategy | Recurrence Rate | Notes |
|---|---|---|
| Surgical Excision Alone | 45% – 100% | Almost guaranteed to return, often larger. |
| Steroid Injections Alone | 9% – 50% | Requires multiple sessions; 50-100% response rate. |
| Surgery + Corticosteroids | < 50% | Significant improvement over surgery alone. |
| Surgery + Radiotherapy | 0% – 8.6% | The most effective protocol for recalcitrant keloids. |
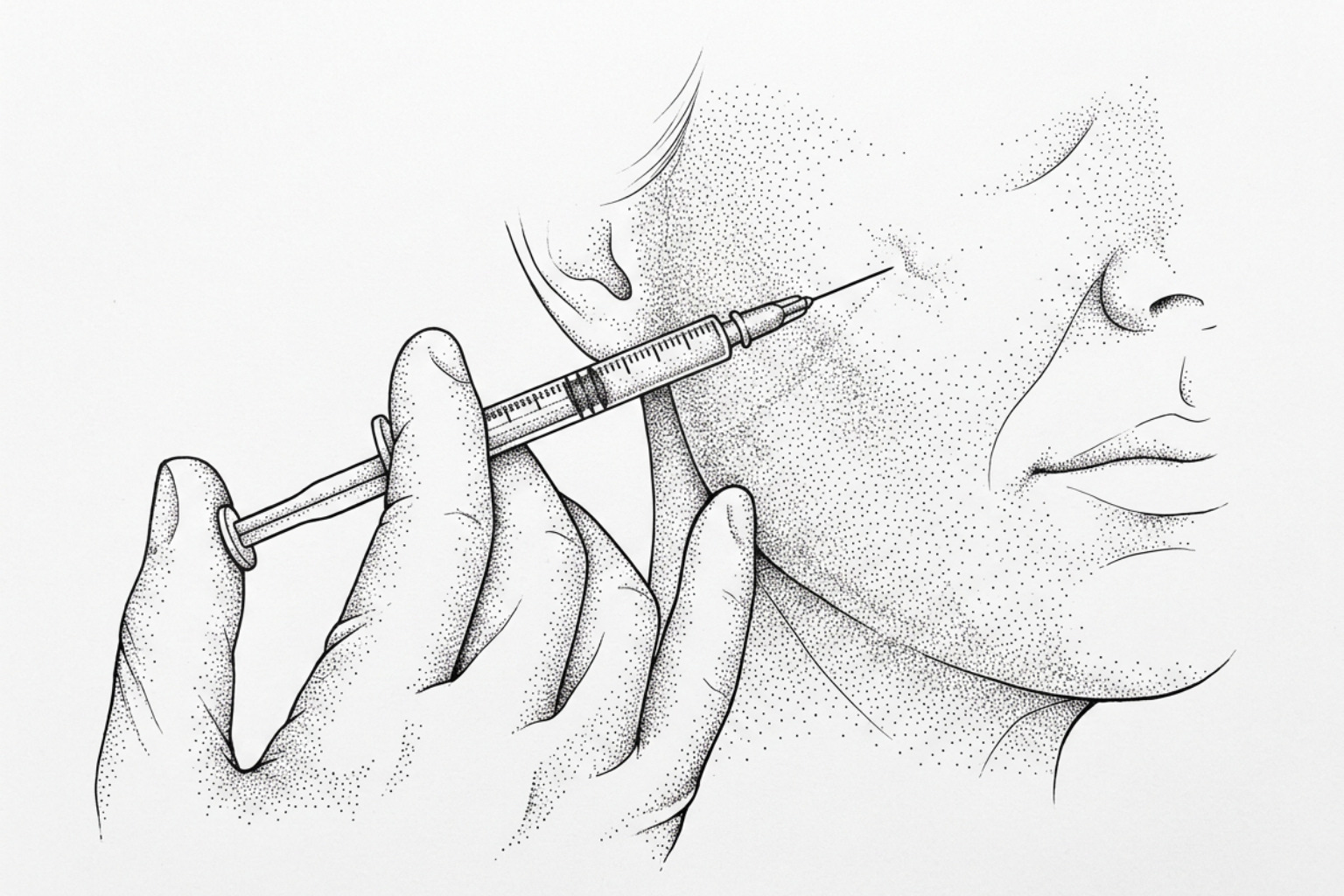
Corticosteroid Injections and Cryotherapy Protocols
Intralesional corticosteroid injections (usually triamcinolone acetonide) are a first-line medical treatment. These injections work by suppressing inflammation and inhibiting fibroblast proliferation.
- Frequency: Typically administered every 3 to 6 weeks for up to six months.
- Combinations: Combining steroids with 5-Fluorouracil (5-FU), a chemotherapy agent, has been shown to increase efficacy in steroid-resistant keloids.
- Cryotherapy: Freezing the keloid with liquid nitrogen before injecting steroids can soften the tissue, making the injection more effective and less painful.
For more on how light-based therapies assist this process, see Laser For Keloid Scars.
Surgical removal plus radiation
For large or painful abdominal keloids, surgical removal may be necessary. To prevent the keloid from returning with a vengeance, surgeons utilize "adjuvant" (extra) therapies immediately following the procedure.
The most successful protocol involves Superficial Radiation Therapy (SRT) or Brachytherapy. High-dose radiation (HDR) brachytherapy, delivered within 7 to 24 hours of surgery, targets the overactive fibroblasts before they can begin the "overhealing" process again. A systematic review of over 3,000 keloids found that HDR brachytherapy achieved a recurrence rate of just 10.5%, compared to over 22% for external beam radiation.
Specialized Management of Umbilical and Perineal Keloids
Keloids in the "belly button" (umbilicus) or the perineal area (lower abdomen/mons pubis) present unique anatomical challenges.

Addressing Post-Abdominoplasty Complications
Following a "tummy tuck," patients may develop keloids along the long horizontal incision or around the repositioned umbilicus. A rare but documented complication is a "sunken umbilicus," where the belly button becomes buried under keloid tissue.
Prevention is key here. Surgeons often use progressive tension sutures (PTS) to distribute the mechanical load across the abdominal wall, reducing the tension on the skin surface. If a keloid does form, Non-Invasive Keloid Removal methods should be started as soon as the wound is fully epithelialized.
Treatment Principles for Perineal and Mons Pubis Keloids
Keloids in the mons pubis or lower abdominal folds can be particularly debilitating, causing pain during movement or interference with intimacy. These areas are prone to moisture and friction, which can exacerbate inflammation.
A successful clinical approach for these sensitive areas includes:
- Wide Local Excision: Removing the keloid with a 3-5mm margin of healthy tissue.
- No-Touch Technique: Minimizing micro-trauma to the skin edges during surgery to prevent triggering new keloid growth.
- Post-Operative Radiation: Initiating electron beam therapy on "Day 1" post-surgery.
- Staged Procedures: For very large masses, clinicians may recommend removing the keloid in stages (6 months apart) to allow the skin to heal without excessive tension.
Frequently Asked Questions about Abdominal Keloids
When is a biopsy necessary for an abdominal scar?
While most doctors can diagnose a keloid simply by looking at it, a biopsy is necessary if the scar looks atypical, grows rapidly, or develops an open sore (ulceration). The primary goal of a biopsy in these cases is to rule out skin cancers, such as dermatofibrosarcoma protuberans (DFSP), which can mimic the appearance of a keloid.
Can abdominal keloids turn into cancer?
No. Keloids themselves are benign (non-cancerous) fibrous growths. They do not transform into malignancy. However, because they can look similar to certain rare skin cancers, any suspicious growth should be evaluated by a dermatologist.
What is the typical timeline for treatment results?
Keloid reduction is a marathon, not a sprint.
- Silicone: 2 to 4 months for visible softening.
- Injections: 3 to 6 months of monthly sessions.
- Radiation/Surgery: 15 to 36 months of follow-up are required to confirm the keloid is truly "cured," as recurrence can happen years later.
Choosing the Right Treatment Approach
Successfully achieving abdomen keloid scar reduction requires a combination of patience, clinical expertise, and a multi-modal treatment plan. While surgery alone often fails, the combination of surgical excision with modern radiotherapy or aggressive corticosteroid protocols offers high success rates.
For those in the early stages of healing, prioritizing Abdomen Scar Reduction Methods like silicone sheeting and sun protection is essential. Protecting the scar from UV rays is particularly important, as sunlight can permanently darken keloid tissue, making it more prominent.
If you are concerned about a growing abdominal scar, consider a professional Scar Assessment to determine if you are dealing with a keloid or a hypertrophic scar. Early intervention is the most effective way to break the cycle of "overhealing" and regain comfort.
Works Cited
- Berman, B., Maderal, A., & Raphael, B. (2017). "Keloids and Hypertrophic Scars: Pathophysiology, Classification, and Treatment." Dermatologic Surgery, 43(Suppl 1), S3-S18. https://pubmed.ncbi.nlm.nih.gov/27347634/
- van Leeuwen, M. C., et al. (2015). "Surgical Excision with Adjuvant Irradiation for Treatment of Keloid Scars: A Systematic Review." Plastic and Reconstructive Surgery Global Open, 3(7), e440.
- Ogawa, R. (2017). "Keloid and Hypertrophic Scars Are the Result of Chronic Inflammation in the Reticular Dermis." International Journal of Molecular Sciences, 18(3), 606.
- Ogawa, R. (2022). The Most Current Algorithms for the Treatment and Prevention of Hypertrophic Scars and Keloids: A 2020 Update. Plastic and Reconstructive Surgery, 149(1), 79e-94e. https://pmc.ncbi.nlm.nih.gov/articles/PMC8687618/
- Kim, S. W., et al. (2021). "Management of Keloid Scars: Noninvasive and Invasive Treatments." Archives of Plastic Surgery, 48(2), 149-157.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.