The Biological Roadmap of Your Healing Scars
Keloid scars develop through predictable biological stages — but in predisposed individuals, each stage goes wrong in specific ways. Discover the science behind keloid formation and what it means for treatment.
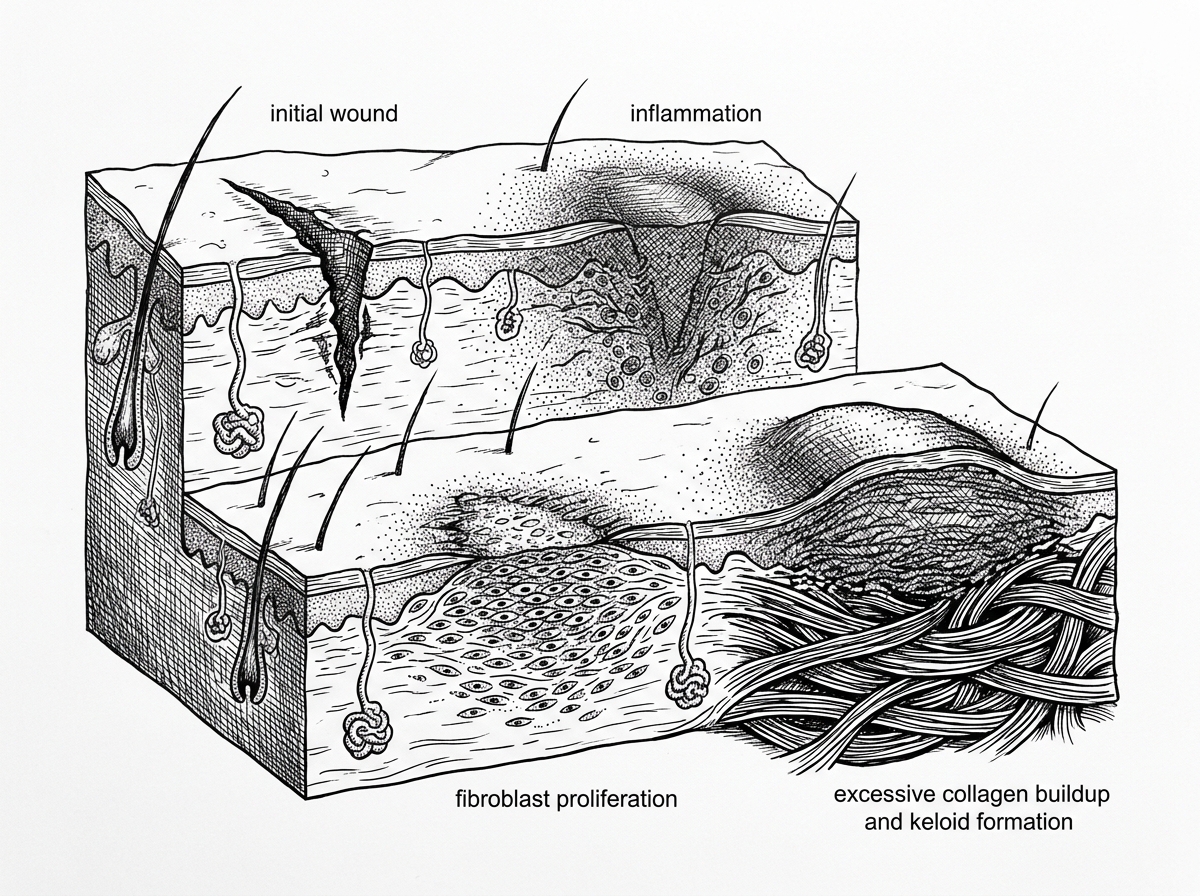
How Keloid Scars Develop Over Time
Keloid scar formation stages follow a predictable biological sequence — but in people with a genetic predisposition, that sequence goes wrong in specific, measurable ways.
Here is a quick overview of how keloid scars develop:
- Hemostasis (minutes to hours) - Bleeding stops; a fibrin clot forms at the wound site
- Inflammation (days 1-14) - Immune cells clean the wound; growth factors are released
- Proliferation (days 3-30) - Fibroblasts migrate in and begin laying down collagen
- Remodeling (weeks 4 to 12+ months) - Collagen is reorganized and the scar matures
- Pathological deviation (months to years post-injury) - In keloid-prone individuals, fibroblasts remain overactive, collagen synthesis continues far beyond wound closure, and the scar grows beyond the original wound margins
In normal wound healing, the remodeling phase brings scar formation to a controlled stop. In keloid formation, that stop signal fails. Research indicates that collagen synthesis in keloids can be 20 times greater than in healthy skin — and three times greater than in hypertrophic scars, which are a related but distinct condition.
The timeline is often slow and unpredictable. Evidence suggests keloids can take anywhere from 3 to 12 months to become visible, and roughly 20% of keloids do not appear until more than a year after the original injury.
Understanding why this happens — at the cellular and molecular level — is the foundation for understanding how keloids can be managed.
Normal Healing vs. Keloid Formation
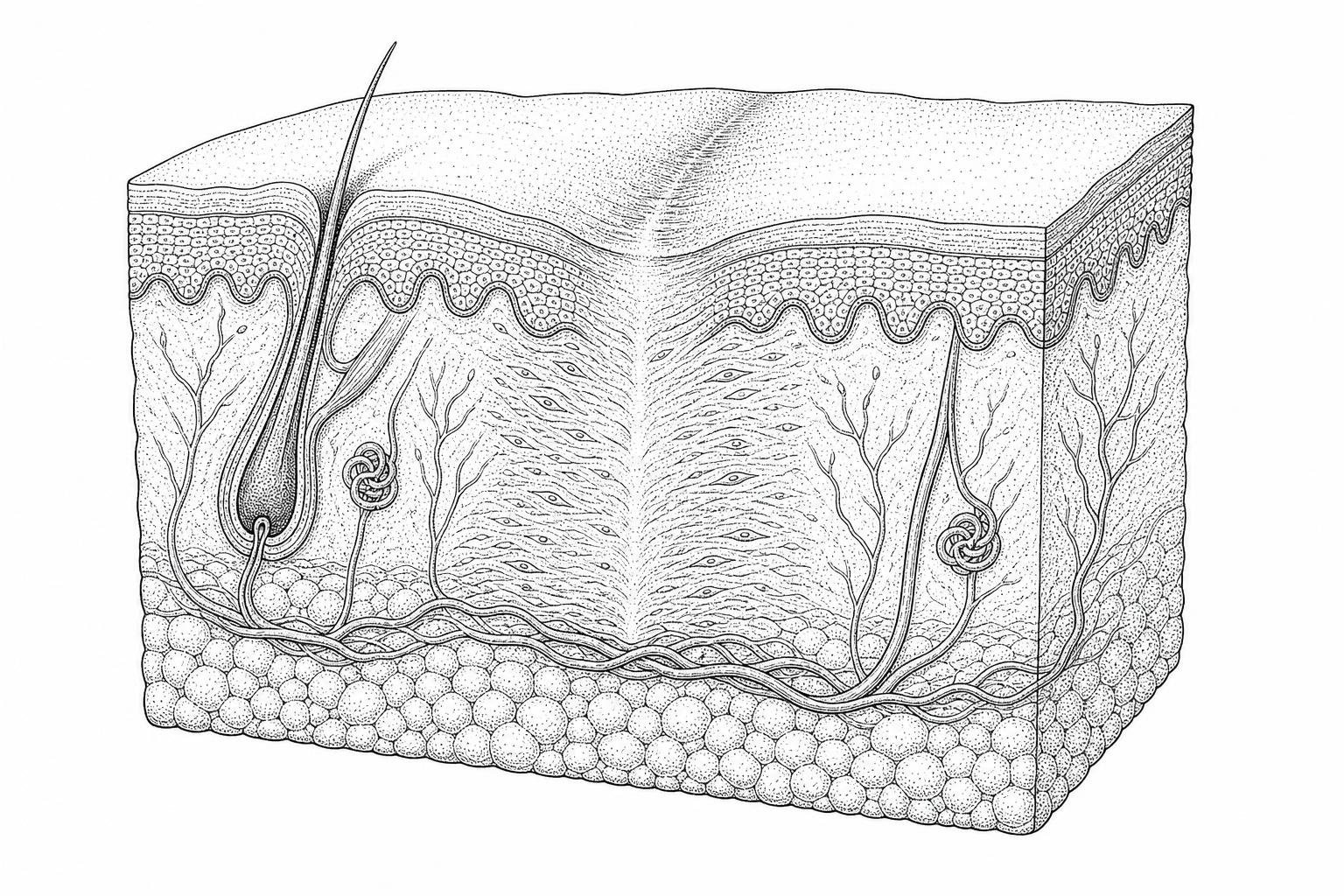
To understand why keloid scar formation stages deviate from the norm, it is necessary to examine the standard mechanisms of cutaneous repair. Wound healing is a highly orchestrated physiological process designed to restore the skin's barrier function. However, when the regulatory signals that govern this process fail, the result is pathological fibrosis—the excessive deposition of connective tissue.
The primary distinction in wound outcomes lies between a "mature" flat scar, a hypertrophic scar, and a keloid. While hypertrophic scars and keloids both represent overgrowths of tissue, their biological behaviors are markedly different.
Comparing Keloid and Hypertrophic Scars
| Feature | Hypertrophic Scar | Keloid Scar |
|---|---|---|
| Onset | Usually within 4–8 weeks post-injury | Months to years post-injury |
| Growth Boundary | Remains within the original wound margins | Extends beyond the original wound boundaries |
| Regression | Often regresses spontaneously over 1–2 years | Rarely regresses; may grow indefinitely |
| Collagen Synthesis | 3x greater than healthy skin | 20x greater than healthy skin |
| Site Predilection | Areas of high tension (joints, back) | Earlobe, chest, shoulders, upper back |
The Role of Hemostasis and Inflammation
In the first 24 hours (hemostasis), a fibrin clot forms to stop bleeding and provide a scaffold for migrating cells. During the subsequent inflammatory response (days 1 to 14), neutrophils and macrophages infiltrate the site. Macrophages are particularly critical; they act as the "conductors" of the healing process, releasing cytokines that signal the next phase. In keloid-prone tissue, research suggests a "Th2 immune shift," where specific inflammatory signals (IL-4 and IL-13) promote excessive fibrogenesis rather than a controlled resolution.
Proliferation and Remodeling
The proliferative phase involves angiogenesis (the formation of new blood vessels) and re-epithelialization. Fibroblasts migrate to the site to synthesize the extracellular matrix (ECM). In normal healing, the remodeling phase follows, where Type III collagen is replaced by stronger Type I collagen, and the scar achieves roughly 80% of its original tensile strength by 10 weeks. In keloids, this remodeling phase is effectively bypassed or delayed, leading to the "tongue-like" advancing edge characteristic of invasive growth. For a deeper dive into these clinical distinctions, the StatPearls review on Hypertrophic Scarring Keloids provides an authoritative overview.
Molecular and Cellular Mechanisms of Keloid Scar Formation Stages
At the heart of the keloid scar formation stages is a profound dysregulation of the fibroblast—the cell responsible for building skin structure. In a keloid, these fibroblasts behave similarly to benign tumor cells: they proliferate faster, live longer, and are resistant to apoptosis (programmed cell death).

The Role of TGF-beta and SMAD Signaling
The most significant molecular driver of keloid formation is the Transforming Growth Factor-beta (TGF-β) pathway. Evidence shows that keloid tissue overexpresses TGF-β1 and TGF-β2, which stimulate collagen production, while under-expressing TGF-β3, which typically helps reduce scarring. These signals are processed via SMAD proteins, which enter the cell nucleus to "turn on" collagen genes. In keloids, this pathway remains permanently "on," leading to a massive accumulation of the extracellular matrix.
Apoptosis Resistance and Immune Dysregulation
Normally, once a wound is closed, the "workhorse" cells (myofibroblasts) should die off. In keloids, these cells persist. This resistance to cell death, combined with a persistent inflammatory environment rich in M2 macrophages, creates a feedback loop of continuous growth. Recent insights into these advanced therapeutic strategies and pathogenesis suggest that targeting these specific signaling pathways may be the key to future treatments.
Clinical Identification of Early Keloid Scar Formation Stages
Early detection is vital for successful management. The first indicators often appear 3 to 12 months after the skin is broken.
- Erythema: The scar remains persistently red or purple long after the wound has closed.
- Pruritus (Itching): Statistics show that 86% of patients with keloids complain of itching, caused by the release of histamine and other inflammatory mediators within the dense tissue.
- Pain and Tenderness: Approximately 46% of patients experience physical pain or a burning sensation as the expanding tissue puts pressure on local nerves.
- Elevation: The scar begins to feel firm, rubbery, and starts to rise above the surrounding skin level.
If you notice these early signs, exploring non-invasive keloid removal options early in the process may prevent the need for more aggressive surgery later.
Cellular Deviations in Keloid Scar Formation Stages
The biological "math" of a keloid is startling. While a hypertrophic scar produces about three times the collagen of healthy skin, a keloid produces 20 times that amount. This is not just a matter of volume; the structure is also different. Keloid collagen consists of thick, haphazard, "glassy" bundles that lack the organized orientation seen in normal scars.
Furthermore, emerging research has highlighted the role of lipid metabolism and mechanotransduction. Keloid tissue has been found to have 60% higher triglyceride levels than normal skin, which may fuel chronic inflammation. Mechanotransduction refers to how skin cells respond to physical tension; in keloid-prone areas like the chest or shoulders, high skin tension activates "piezo" channels on the cell surface, signaling the fibroblasts to produce even more collagen in a misguided attempt to "reinforce" the area. You can find more peer-reviewed research on these cellular mechanisms to better understand the complexity of the condition.
Clinical Determinants and Risk Factors for Pathological Scarring
Not everyone is equally susceptible to keloids. The risk is determined by a combination of genetics, age, and the location of the injury.
Genetic Predisposition and Skin Type
Epidemiological data shows that keloids are most common in individuals with darker skin pigmentation (Fitzpatrick scales IV-VI). The incidence in African, Asian, and Hispanic populations ranges from 4.5% to 16%. Genetic studies have identified specific markers, such as the NEDD4 gene, which appear to increase susceptibility. Family history is a strong predictor; over 50% of people with keloids report a relative with the same condition.
Age and Hormonal Factors
Keloids most frequently develop between the ages of 10 and 30. There is a notable peak during puberty and pregnancy, suggesting that growth hormones and endocrine factors play a significant role in stimulating fibroblast activity. Conversely, keloids are rare in the very young and the elderly.
Anatomical Distribution and High-Tension Regions
Keloids rarely occur on the palms of the hands, soles of the feet, or the face (except the jawline). Instead, they have a strong predilection for "high-tension" areas:
- The Earlobe: Often triggered by piercings.
- The Chest and Sternum: Frequent sites for post-acne keloids.
- The Shoulders and Upper Back: Areas where skin is constantly stretched by movement.
Understanding these risk factors and regional patterns is essential for those considering elective procedures like tattoos or piercings.
Evidence-Based Management and Therapeutic Strategies
Treating a keloid is notoriously difficult because of the high recurrence rate—up to 100% when surgical excision is used alone. Therefore, modern clinical consensus favors multimodal therapy.
First-Line Treatments
- Intralesional Corticosteroids: Injections of Triamcinolone acetonide (TAC) remain the "gold standard." These help flatten the scar by inhibiting fibroblast proliferation and reducing collagen synthesis. Success rates for significant flattening range from 50% to 100%.
- Silicone Gel Sheeting: This non-invasive method works by hydrating the scar and reducing tension. It is most effective when worn for 12–24 hours a day for at least 2 to 3 months.
- Pressure Therapy: Especially effective for earlobe keloids, pressure clips or garments (applying 15-40 mmHg of pressure) can help "starve" the keloid of oxygen and nutrients, slowing its growth.
Advanced and Adjuvant Therapies
- Cryotherapy: Freezing the tissue with liquid nitrogen can cause the keloid to slough off. Recent techniques using intralesional cryo-needles have shown volume reductions of over 50%.
- 5-Fluorouracil (5-FU): Originally a chemotherapy drug, low-dose injections of 5-FU can be used alone or combined with steroids to stop the rapid cell division of keloid fibroblasts.
- Laser Therapy: Pulsed-dye lasers (PDL) target the blood vessels supplying the keloid, reducing its redness and size. For those with acne-related scarring, microneedling or specialized laser treatments may be considered, though caution is required to avoid triggering further keloid growth. More information on laser protocols for keloids is available for those exploring high-tech options.
- Surgical Excision with Radiation: For severe cases, the keloid is surgically removed, followed immediately (within 24–72 hours) by superficial radiation therapy. This combination reduces the recurrence rate to less than 10-20%.
Clinical Considerations in Keloid Pathogenesis and Progression
Temporal Onset Post-Injury
The timeline for keloid scar formation stages is much slower than that of a standard scar. While a normal scar might look its "worst" at 4 weeks and then improve, a keloid often doesn't even begin to show until 3 to 12 months post-injury. In roughly 20% of cases, the first signs of elevation or itching appear more than a year after the skin has healed.
Spontaneous Keloid Formation and Minor Trauma
Yes, "spontaneous" keloids are documented, particularly on the chest. However, many medical professionals believe these are often triggered by minor, forgotten traumas—such as an ingrown hair, a pimple, or a small insect bite—that initiated a massive inflammatory response in a predisposed individual.
Mechanisms of Invasive Growth Beyond Wound Margins
Unlike hypertrophic scars, which stay within the "lines" of the injury, keloids are characterized by invasive growth. This happens because keloid fibroblasts migrate laterally into healthy skin. The failure of the remodeling phase means there is no "off switch," allowing the tissue to expand like a slow-growing, benign tumor.
Conclusion
The journey through the keloid scar formation stages is a complex biological process driven by genetics, tension, and cellular overactivity. While keloids do not typically resolve on their own, understanding the biological roadmap allows for more targeted interventions. The key to management is early recognition of symptoms like persistent itching and redness, followed by a multimodal treatment plan tailored to the individual's risk factors.
The long-term prognosis for keloids is best when managed by an interprofessional team of dermatologists and specialists who can monitor for recurrence. If you are concerned about a developing scar, you can complete a professional scar assessment to determine the best path forward for your skin’s health.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- Berman, B., Maderal, A., & Raphael, B. (2017). Keloids and Hypertrophic Scars: Pathophysiology, Classification, and Treatment. Dermatologic Surgery, 43(Suppl 1), S3–S18. https://pubmed.ncbi.nlm.nih.gov/27347634/
- Ogawa, R. (2017). Keloid and Hypertrophic Scars Are the Result of Chronic Inflammation in the Reticular Dermis. International Journal of Molecular Sciences, 18(3), 606. https://pmc.ncbi.nlm.nih.gov/articles/PMC5372622/
- Huang, C., & Ogawa, R. (2020). The Most Current Algorithms for the Treatment and Prevention of Hypertrophic Scars and Keloids. Plastic and Reconstructive Surgery, 146(6), 1256–1269. https://pmc.ncbi.nlm.nih.gov/articles/PMC8687618/
- Shah, M., Foreman, D. M., & Ferguson, M. W. J. (2007). Transforming growth factor beta (TGFβ) and keloid disease. International Journal of Experimental Pathology, 85(1), 7–16. https://pubmed.ncbi.nlm.nih.gov/17660136/
- Gurtner, G. C., et al. (2008). Wound repair and regeneration. Nature, 453(7193), 314–321. https://pubmed.ncbi.nlm.nih.gov/18480812/