The Ultimate Post-Op Guide to Taping and Managing Your C-Section Scar
C-section scar revision ranges from taping techniques to surgical correction. Learn evidence-based post-op strategies to improve your cesarean scar appearance and comfort.
When to Consider C-Section Scar Revision
C-section scar revision is a surgical or minimally invasive procedure that improves the appearance, comfort, and contour of scars left after cesarean delivery.
Here is a quick overview of the most important facts:
| Question | Short Answer |
|---|---|
| What is it? | Excision of scar tissue and layered closure to create a flatter, less visible scar |
| Who is it for? | People with indented, raised, painful, or wide C-section scars |
| When can it be done? | Generally 6-12 months after delivery, once the scar has matured |
| Surgical or non-surgical? | Both options exist — from excision to laser, microneedling, and injections |
| Can it be combined? | Yes — with tummy tuck, liposuction, or other abdominal contouring |
| Will the scar disappear? | No — but it can be significantly improved in appearance and texture |
Cesarean section is the most commonly performed surgery in the United States. Yet the scar it leaves behind is rarely discussed with the same attention given to the birth itself.
For many people, the initial scar is unremarkable. But for others, it heals in ways that are visually noticeable or physically uncomfortable — creating a ridge, shelf, indentation, or raised band of tissue along the lower abdomen.
These outcomes are not simply cosmetic complaints. The way a C-section scar heals is influenced by how the underlying tissue layers were closed during surgery, individual biology, and the body's own wound-healing response. When deeper fascial layers are not precisely reapproximated, the result can be a visible structural deformity — not just surface discoloration.
This guide examines the clinical evidence behind C-section scar revision: what causes poor scar outcomes, who is a suitable candidate, what surgical and non-surgical techniques are available, and what realistic outcomes look like.
How C-Section Scars Affect Your Abdomen
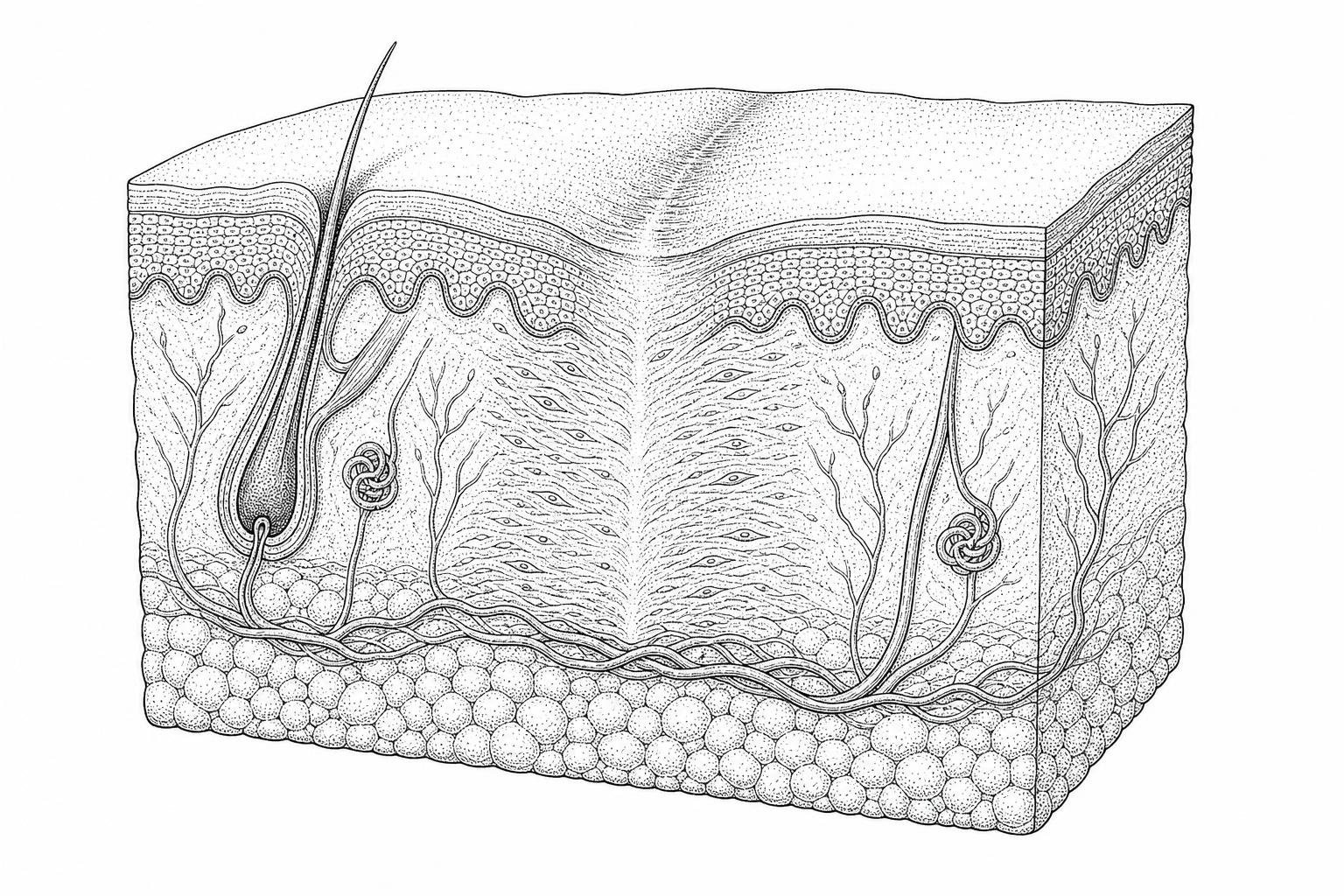
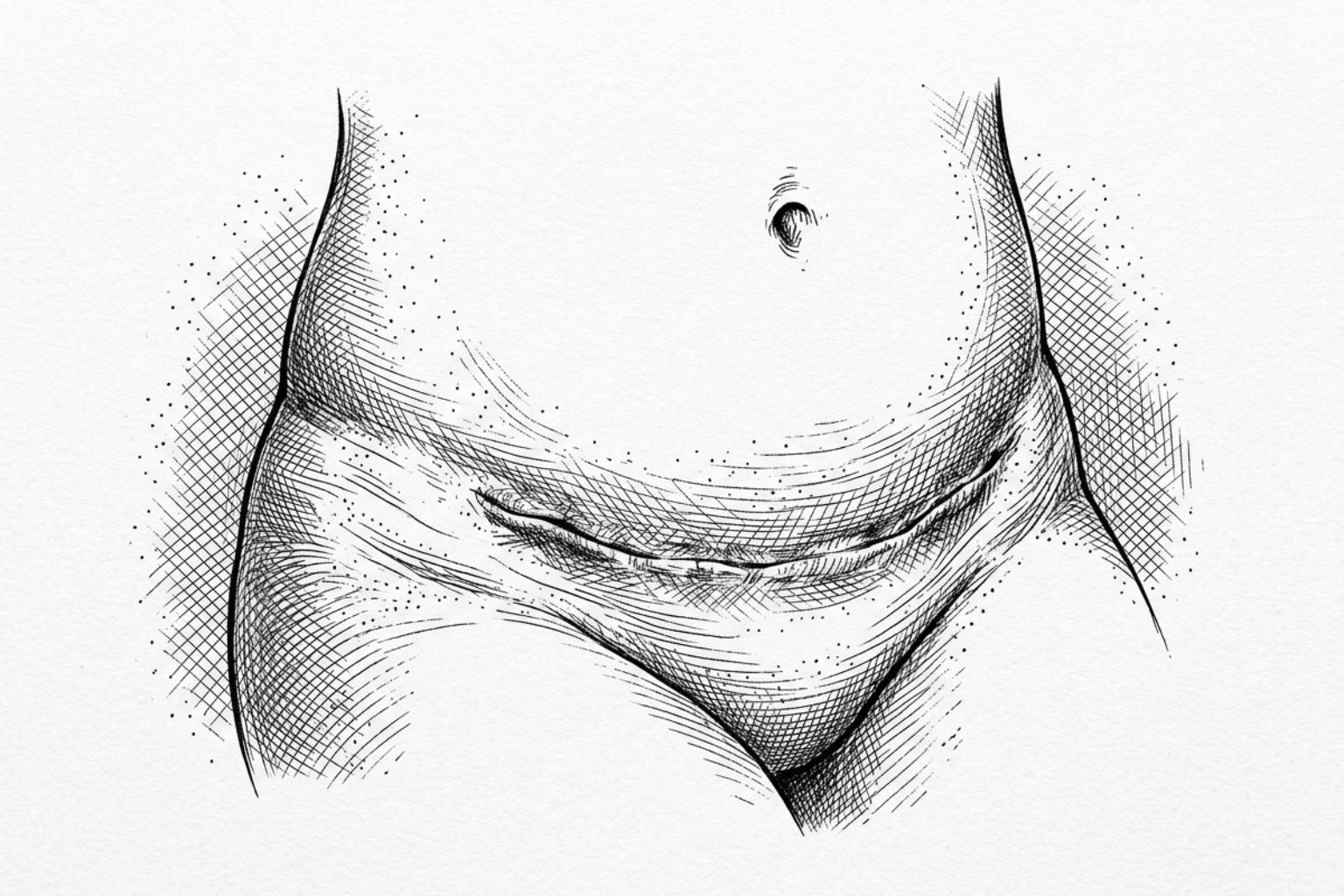
The "C-section shelf" or "pooch" is a common clinical observation where the skin appears to hang over the incision line, or the scar itself looks deeply tethered to the underlying muscle. To understand why this happens, it is necessary to examine the anatomy of the abdominal wall.
The abdominal wall consists of several distinct layers: the skin, subcutaneous fat, the superficial fascia (Scarpa’s fascia), and the deep muscle fascia. During a cesarean delivery, surgeons must navigate these layers quickly to reach the uterus. In many cases, especially during emergency procedures, the focus is on a safe delivery rather than aesthetic closure.
Research into Abdomen Scar Reduction Methods indicates that indented scars often occur because Scarpa’s fascia—the fibrous layer of tissue beneath the skin—is not always sutured closed. When this layer is left unrepaired, the subcutaneous fat can separate, and the skin may heal directly to the underlying muscle fascia. This creates a "tethering" effect where the scar is pulled inward while the fat above it bulges outward, creating the characteristic "shelf."
Furthermore, if the tissue layers are misaligned during closure, "step-offs" occur. This is a visible unevenness where one side of the incision sits higher than the other. Understanding these mechanical causes is essential because surface-level treatments like creams cannot resolve structural tethering; often, a physical release of the adhesion is required.
When Is the Right Time for Revision
Not every C-section scar requires surgical intervention. Clinical indications for c-section scar revision generally fall into two categories: aesthetic dissatisfaction and functional impairment.
Functional issues often include persistent pain, itching, or a sensation of "pulling" during physical activity. In some cases, nerve entrapment within the scar tissue can lead to chronic localized discomfort. More serious internal complications, such as an isthmocele (a defect in the uterine scar), may require specialized gynecological repair rather than a standard skin revision.
Aesthetic indications include hypertrophic scarring (thick, raised red scars) or keloid formation. While both involve an overproduction of collagen, keloids extend beyond the boundaries of the original incision and are more common in individuals with higher melanin levels.
The Importance of Scar Maturation
Timing is a critical factor in the success of any revision. Clinical guidelines suggest waiting at least 6 to 12 months—and ideally up to 18 months—before undergoing surgery. This allows the scar to undergo the full "remodeling phase" of wound healing. During this time, the redness typically fades as the blood supply to the scar decreases, and the tissue softens.
Research into scar revision outcomes indicates that surgical success is highly dependent on the stability of the surrounding tissue. A formal Scar Assessment by a specialist can determine if the tissue has reached sufficient maturity for a successful outcome. Operating too early on an immature, inflamed scar can increase the risk of poor healing or the recurrence of hypertrophic tissue.
Are You a Candidate for Revision
Ideal candidates for this procedure are individuals in good general health who have realistic expectations. Key factors include:
- Stable Weight: Fluctuations in weight can alter the tension on the abdominal skin, potentially compromising the results of the revision.
- Smoking Cessation: Nicotine constricts blood vessels, significantly increasing the risk of wound dehiscence (opening) and infection. Most surgeons require patients to be nicotine-free for at least four weeks before and after surgery.
- Family Planning: If you are planning future pregnancies, it is generally advised to postpone scar revision. A subsequent C-section will involve a new incision through the same area, likely undoing the results of the revision.
- Skin Elasticity: The quality of the surrounding skin determines how well the new incision can be closed without excessive tension.
Surgical Options for C-Section Scars
When non-invasive methods are insufficient, surgical revision offers the most definitive results for correcting structural issues like tethering or wide, depressed scars.

Surgical Excision and Layered Closure
The primary technique involves the precise excision of the old scar tissue. Once the damaged tissue is removed, the surgeon carefully undermines the surrounding skin to relieve tension. The key to preventing a recurrence of the "shelf" is a layered closure. This involves suturing each anatomical layer—fascia, fat, and skin—individually. By repairing Scarpa’s fascia, the surgeon ensures that the fat remains evenly distributed and the skin does not adhere to the muscle.
Tension Reduction Techniques: Z-Plasty and W-Plasty
In cases where the scar is tight or restricting movement, advanced techniques like Z-plasty or W-plasty may be used. These methods involve creating small triangular skin flaps that are rearranged to change the direction of the scar and redistribute tension. This can make the scar less conspicuous by aligning it more closely with the natural skin creases (Langer’s lines). For a deeper look at these methods, see our Surgical Scar Revision Complete Guide.
Combining Scar Revision with Body Contouring
Many patients choose to combine c-section scar revision with other abdominal procedures to achieve a more comprehensive result.
- Mini-Tummy Tuck: If there is a small amount of excess skin and fat below the navel, a mini-abdominoplasty can remove the scar and the "pooch" simultaneously.
- Liposuction: This can be used to thin the fatty tissue around the scar, further smoothing the abdominal contour.
- Hernia Repair: If a ventral hernia has developed at the site of the C-section, it can often be repaired during the same surgical session.
Non-Surgical Options and Add-On Treatments
For patients with mild scarring or those who wish to avoid surgery, several non-invasive options can improve scar texture and color.
Energy-Based Treatments
Laser therapy is a leading non-surgical option. Fractional lasers create microscopic columns of injury in the skin, which triggers the body's natural repair mechanism and stimulates new collagen production. This can soften thick scars and improve overall texture. Detailed information on these technologies can be found in our guides on C Section Scar Laser and the Non Invasive C Section Scars Guide.
Radiofrequency (RF) microneedling is another effective tool. It combines physical needling with thermal energy to remodel the deeper dermal layers, which can be particularly helpful for tightening slightly loose skin around the incision.
Injectable Treatments
For hypertrophic or keloid scars, corticosteroid injections are often the first line of defense. These injections help break down the excess collagen fibers, causing the scar to flatten and soften over a series of treatments. In some cases, hyaluronic acid fillers may be used to "lift" depressed or atrophic scars, though these results are temporary.
Non-Surgical Adjuncts to C-Section Scar Revision
Whether you choose surgery or a less invasive route, topical management is a standard part of clinical care.
- Silicone Gel Sheets: These are considered the gold standard in non-surgical scar management. They work by hydrating the scar and providing slight pressure, which helps regulate collagen production.
- Pressure Therapy: Compressive garments can help reduce swelling and limit the blood flow to an overactive scar.
- Topical Creams: Ingredients like onion extract or specific peptides may assist in soothing the area, as discussed in our Postpartum Scar Reduction Cream Guide.
Recovery After C-Section Scar Revision
Recovery from a standalone c-section scar revision is typically much faster than the original C-section. Most patients can return to light desk work within a few days, though full tissue remodeling takes significantly longer.
| Timeframe | Healing Phase | Clinical Milestones & Restrictions |
|---|---|---|
| 0 - 48 Hours | Inflammatory | Swelling, redness, and mild discomfort. Keep the area dry. |
| 1 - 2 Weeks | Proliferative | Stitches may be removed (if not dissolvable). No heavy lifting (>10 lbs). |
| 2 - 6 Weeks | Early Remodeling | Swelling subsides. Gentle exercise can usually resume. Initial scar appears red/pink. |
| 3 - 6 Months | Maturation | Scar begins to fade. Collagen continues to organize. Sun protection is vital. |
| 1 Year+ | Final Result | Scar reaches maximum strength and fades to a pale, flat line. |
Effective Post Surgery Scar Care is essential during these phases. Standard clinical practice involves advising patients to avoid direct sun exposure on the scar for at least one year, as UV rays can cause permanent hyperpigmentation (darkening) of the healing tissue.
Clinical Considerations and Patient Consultation Parameters
How long is the recovery period before returning to exercise?
Most patients can resume walking and light activity immediately. However, core-strengthening exercises and heavy lifting should typically be avoided for 4 to 6 weeks to prevent the new incision from stretching or widening. Always follow your surgeon's specific clearance.
Does insurance cover the cost of scar revision?
In most cases, c-section scar revision is considered a cosmetic procedure and is not covered by insurance. However, if the revision is medically necessary—for example, to treat chronic pain, nerve entrapment, or a documented functional impairment—partial coverage may be possible. You should consult with both your provider and insurance carrier for a clinical determination.
Can a revised scar disappear completely?
No surgical procedure can completely erase a scar. The goal of revision is to replace a wide, thick, or indented scar with a thinner, flatter, and more discreet line that blends into the surrounding skin.
Clinical Summary
A C-section scar is a permanent mark of a significant life event, but it does not have to be a source of physical discomfort or self-consciousness. By understanding the underlying anatomy of the "shelf" and the biological timeline of wound healing, patients can make informed decisions about their care.
Whether through advanced surgical excision or non-invasive laser remodeling, modern clinical techniques offer significant improvements in abdominal contour and scar quality. If you are considering a change, a professional Scar Assessment is the first step toward achieving a result that helps you feel more comfortable in your own skin.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Works Cited
- American College of Obstetricians and Gynecologists (ACOG). (2024). Cesarean Birth. ACOG Clinical Practice Guideline. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2024/03/cesarean-birth
- Gauglitz, G. G., Korting, H. C., Pavicic, T., Ruzicka, T., & Jeschke, M. G. (2011). Hypertrophic Scarring and Keloids: Pathomechanisms and Current and Emerging Treatment Strategies. Molecular Medicine, 17(1–2), 113–125. https://pmc.ncbi.nlm.nih.gov/articles/PMC3022978/
- Tower, A. M., & Frishman, G. N. (2013). Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications. Journal of Minimally Invasive Gynecology, 20(5), 562–572. https://pubmed.ncbi.nlm.nih.gov/23680518/
- Mustoe, T. A., et al. (2002). International Clinical Recommendations on Scar Management. Plastic and Reconstructive Surgery, 110(2), 560–571. https://pubmed.ncbi.nlm.nih.gov/12142678/