The Best Chemical Peel for Body Scars: A Complete List
Comparing TCA, glycolic, and mandelic acid peels for body scars. Each acid matched by Fitzpatrick skin type, scar depth, and body region to help you find the safest, most effective option.

For readers asking what the best chemical peel for body scars is, the evidence-based answer is that there is no single best option for every scar. The appropriate peel depends on scar type, skin tone, body location, and peel depth.
Here is a quick-reference summary for those comparing options:
| Acid Type | Peel Depth | Best For | Skin Tone Suitability |
|---|---|---|---|
| Glycolic acid (AHA) | Superficial | Mild acne scars, uneven tone | Fitzpatrick I-IV |
| Lactic acid (AHA) | Superficial | Sensitive skin, mild discoloration | Fitzpatrick I-VI |
| Salicylic acid (BHA) | Superficial | Acne-related scarring, oily skin | Fitzpatrick I-IV |
| Mandelic acid (AHA) | Superficial-medium | Darker skin tones, PIH, acne scars | Fitzpatrick IV-VI |
| TCA (trichloroacetic acid) | Medium-deep | Atrophic scars, surgical scars, texture | Fitzpatrick I-IV (with caution) |
| Phenol | Deep | Severe scarring | Fitzpatrick I-III only |
Scars on the body, whether caused by acne, surgery, burns, or trauma, can persist for years and often respond poorly to routine topical care alone. One reason is anatomical. Body skin is generally thicker than facial skin in many regions, especially on the back and shoulders, which can limit the visible effect of low-potency over-the-counter products on established scar texture.
Chemical peels work through controlled chemical exfoliation. Depending on the acid used and its concentration, they can loosen corneocyte adhesion in the epidermis, increase epidermal turnover, and in deeper peels create a controlled injury that triggers wound-healing responses, including fibroblast activity and collagen remodeling. General clinical guidance from the American Academy of Dermatology and peer-reviewed reviews supports this mechanism, although high-quality body-scar-specific trials remain limited.
That limitation matters. Evidence is stronger for facial acne scarring and dyschromia than for scars on the trunk or limbs. Many recommendations for body scars are therefore based on a combination of acne-scar studies, pigment-disorder literature, and specialist clinical practice rather than large randomized trials focused specifically on body sites.
The wrong peel can also worsen the problem. In darker skin tones, excessive inflammation can trigger post-inflammatory hyperpigmentation (PIH). Medium-depth and deep peels also carry a higher risk of prolonged erythema, delayed healing, and secondary pigment change.
The sections below review what clinical evidence and current dermatologic practice suggest about acid type, peel depth, skin tone, and treatment region, so decisions can be based on mechanism and safety rather than marketing claims.
How chemical peels work on body scars
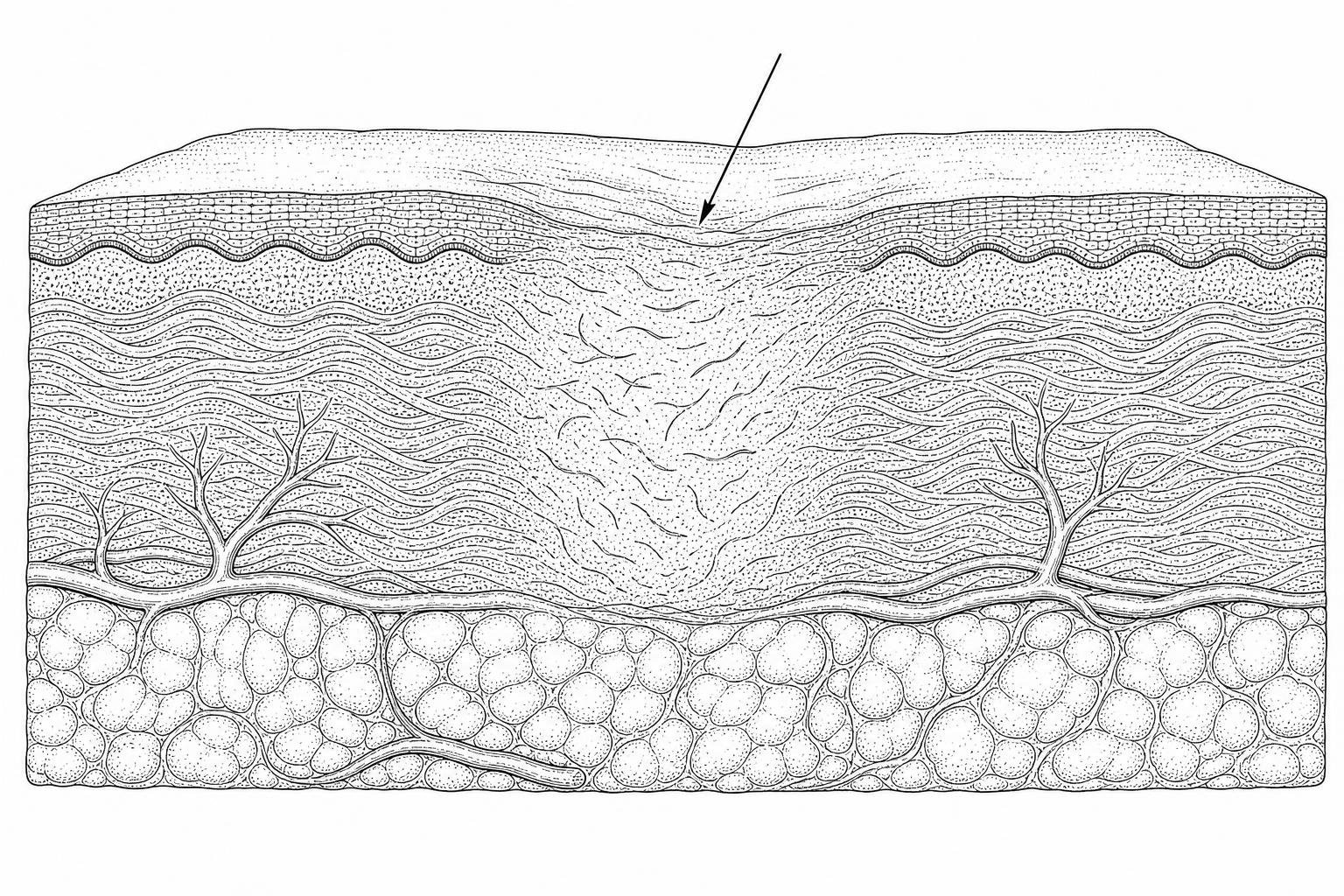
Chemical peels help body scars in two main ways: surface resurfacing and deeper remodeling.
At the surface, acids loosen the bonds between dead keratinocytes in the epidermis. This speeds cell turnover and can gradually reduce rough texture, dullness, and excess pigment left behind by acne, folliculitis, injury, or surgery. This is why superficial peels are often useful for body acne marks and flat discoloration.
Deeper in the skin, some peels create a controlled injury that triggers wound-healing pathways. Fibroblasts, the cells that build collagen and other extracellular matrix proteins, become more active during repair. Over time, that remodeling may soften irregular texture and partially improve shallow atrophic scars. That is the theory behind using medium-depth peels for depressed or texturally uneven scars, and it is supported by acne-scar literature more strongly than by body-scar-specific trials.
This distinction matters. A peel can improve:
- Surface roughness
- Uneven pigmentation
- Mild textural irregularity
- Some shallow depressed scarring
A peel is less reliable for:
- Thick hypertrophic scars
- Keloids
- Deep tethered scars
- Scars with major volume loss
In other words, a chemical peel is not a magic eraser. It is more like a controlled reset button for the upper skin layers, with some collagen signaling underneath. Clinical reviews suggest superficial peels can improve tone and mild textural issues with limited downtime, while medium peels may produce better scar revision at the cost of longer recovery. For a broader overview of how this fits into scar management, see chemical peel scar revision.
Why lotions often fail is simpler than marketing makes it sound. Most body creams mainly hydrate the stratum corneum, the outer barrier layer. Hydration can temporarily soften roughness and improve the look of dry scar tissue, but it does not usually reach the depth needed to reorganize collagen. That is especially true on the back, shoulders, and chest, where skin is thicker and more sebaceous.
Which Acid Works Best for Your Body Scars?
No single acid is the universal answer. The best chemical peel for body scars depends on the problem being treated, the depth targeted, the body site, and the patient's risk of irritation or dyspigmentation.
Evidence for chemical peels is stronger for facial acne scarring than for scars on the trunk or limbs. For many body scars, recommendations are extrapolated from acne-scar studies, pigment-disorder literature, and clinical experience rather than large body-specific randomized trials.
- Glycolic acid (AHA)
- Small molecular size allows relatively efficient epidermal penetration.
- Best suited to mild post-acne marks, rough texture, and uneven tone.
- Often used in superficial peels and repeated sessions.
- Can be more irritating than lactic or mandelic acid in some patients.
Clinical reviews support glycolic acid for acne-related discoloration and mild textural irregularity, but high-quality evidence for established body-scar revision remains limited.
- Lactic acid (AHA)
- Generally milder than glycolic acid.
- Also acts as a humectant, which may improve tolerability in dry or sensitive skin.
- Useful for mild discoloration and rough patches.
Lactic acid is often used when a conservative resurfacing approach is preferred.
- Salicylic acid (BHA)
- Oil-soluble, so it penetrates into follicles.
- Helpful for acne-prone areas such as the back and chest.
- Best for post-acne marks, clogged pores, and ongoing breakouts that are contributing to new scars.
It is generally more useful for prevention plus treatment of acne-related marks than for remodeling mature surgical scars.
- Mandelic acid (AHA)
- Larger molecular size means slower penetration.
- Often better tolerated in sensitive skin and in darker skin tones.
- Commonly used when post-inflammatory hyperpigmentation risk is a major concern.
This acid is often chosen when the main goal is gradual brightening and smoothing rather than aggressive resurfacing.
- Trichloroacetic acid (TCA)
- Used in medium-depth peels and, at higher concentrations, can reach deeper structures.
- More capable than superficial acids for textural change and some shallow atrophic scar improvement.
- Carries greater risk of prolonged redness, dyspigmentation, delayed healing, and complications if used incorrectly.
For body scars, TCA requires caution. Safety depends on concentration, pH, skin preparation, body site, and aftercare, not on marketing terms. Medium-depth and high-strength TCA peels are generally better suited to clinician supervision than home use. For general educational coverage, see chemical peels.
- Phenol
- Deep peel agent with the greatest downtime and risk.
- Usually reserved for severe facial photodamage or scarring in carefully selected patients.
- Rarely appropriate for routine body-scar treatment.
For most body scars, phenol is not a practical first-line option.
- Phytic acid
- A superficial peeling agent sometimes included in combination formulations.
- Primarily studied for dyschromia and gentle exfoliation rather than established scar remodeling.
- May be considered when irritation tolerance is low, but evidence for meaningful body-scar revision is weak.
Chemical Peel Selection by Fitzpatrick Skin Type in Body Scar Treatment
Choosing by skin tone is not optional. It is a safety issue.
The Fitzpatrick scale classifies skin by how easily it burns or tans, from I to VI. In darker skin tones, inflammation after a peel can stimulate melanocytes and cause post-inflammatory hyperpigmentation. In some cases, the discoloration becomes more noticeable even if the scar texture improves.
General patterns used in clinical practice:
- Fitzpatrick I-III: broader peel options, though stronger peels still carry risk
- Fitzpatrick IV-VI: more caution, slower escalation, and preference for gentler acids or specialist supervision
For darker skin tones:
- Mandelic acid is often favored because it penetrates more slowly and may reduce irritation risk.
- Lactic acid is also commonly used when sensitivity is a concern.
- Medium-depth TCA may still be used in selected cases, but usually only with careful priming, test spots, and expert oversight.
For sensitive skin:
- Lactic acid is often the most conservative starting point.
- Low-strength mandelic acid can also be reasonable.
- Combining multiple strong acids without supervision increases the risk of barrier injury and dyspigmentation.
More detail on pigmentation risks and scar-focused peel selection is available in chemical peel scars.
Which peel suits your scar type
Scar type matters as much as acid type.
Atrophic scars
- These are depressed scars caused by collagen loss.
- Medium peels, especially TCA-based approaches, may help shallow atrophic scars by stimulating remodeling.
- Deep or sharply defined scars often respond better to combination treatment such as microneedling, subcision, or laser resurfacing.
- These are raised scars caused by excess collagen.
- Chemical peels are usually not first-line treatment.
- Silicone therapy, corticosteroid injections, laser therapy, or pressure-based approaches generally have stronger clinical support.
Acne scarring on the body
- Common on the back, shoulders, and chest.
- If active acne is still present, salicylic acid or superficial mixed-acid peels may help reduce both breakouts and residual marks.
- If the problem is mostly shallow textural scarring, glycolic or carefully selected TCA peels may be considered.
Surgical scars
- Flat but discolored scars may respond to superficial peels.
- Textured or depressed scars may need a medium peel or another modality entirely.
- Raised or widened scars often need non-peel approaches.
Striae alba (mature stretch marks)
- Evidence suggests glycolic acid and TCA-based resurfacing may modestly improve texture and appearance in some patients.
- Results are usually partial rather than complete.
- The evidence base is limited, and expectations should remain conservative.
Depth of Penetration: Superficial, Medium, and Deep Peels
Body peels differ not just by acid, but by depth of injury.
| Peel Depth | Typical Reach | Best Uses | Recovery |
|---|---|---|---|
| Superficial | Epidermis | PIH, rough texture, mild acne marks | Usually 1-7 days |
| Medium | Epidermis to papillary dermis | Shallow atrophic scars, more visible texture issues | Often 7-14 days |
| Deep | Mid-reticular dermis | Severe scarring in selected cases | Often 14-21 days or longer |
Superficial peels
- Usually use AHAs or BHAs.
- Best for discoloration, roughness, and mild scar visibility.
- Minimal downtime and lower risk profile.
Medium peels
- Often involve TCA, sometimes in combination formulas.
- Reach beyond the epidermis into the papillary dermis.
- More likely to improve texture, but also more likely to cause prolonged redness, peeling, and pigment change.
Deep peels
- Usually phenol-based.
- Require close medical supervision.
- Not commonly used for routine body-scar revision because recovery is significant and risk is much higher.
Body peels also differ from facial peels because body skin is thicker in some regions and may appear less reactive at the surface, yet healing can be slower in areas with friction, lower relative circulation, or repeated irritation. The chest and shoulders, for example, are common sites of both acne scarring and post-treatment pigment change.
A body-specific peel category exists in clinical practice because treatment below the clavicle is not identical to treatment on the face. Product names and clinic marketing, however, should never replace individualized medical assessment.
Are body chemical peels safe?
At-home body peels exist, but “available” is not the same as “appropriate.”
Home use may be reasonable when:
- The peel is superficial
- The acid strength is low
- The goal is mild discoloration or roughness
- The user follows instructions exactly
- A patch test is done first
Home use is not a good idea when:
- The peel contains high-concentration TCA
- The scar is deep or extensive
- The patient has a history of keloids, PIH, eczema flares, or poor wound healing
- The skin is recently tanned, sunburned, infected, or broken
Important precautions include:
- Patch test before full application
- Avoid retinoids, scrubs, and other exfoliants before and after treatment
- Use broad-spectrum SPF 30+ on exposed treated areas
- Do not peel off shedding skin manually
- Moisturize to support barrier repair
- Stop immediately if blistering, severe pain, gray-white frosting beyond expected level, or signs of infection occur
Neutralization matters too. Some acids self-neutralize over time, while others require active rinsing or a specific neutralizing step depending on the formula. This is one reason generic “leave it on longer for better results” advice is so dangerous.
For professional medium or deep peels, clinicians may use antiviral prophylaxis in selected patients, especially with a history of herpes simplex when relevant to the treatment area. Erythema, swelling, crusting, and temporary darkening are common parts of recovery, but persistent inflammation increases complication risk.
Regional Variations in Body Skin Thickness and Treatment Response
Different body areas respond differently to the same peel.
Back and chest
- Thick, oily, acne-prone skin
- Often suitable for salicylic acid or glycolic acid when acne and PIH dominate
- Can also be treated with medium-depth peels for selected textural scars
- Friction from clothing and sweating can complicate healing
Shoulders and upper arms
- Common site for folliculitis, acne marks, and keratosis pilaris
- Superficial peels often help rough texture and discoloration
- Overly aggressive peels can trigger PIH
Legs
- May heal more slowly than the trunk
- Shaving, dryness, and reduced oil production can increase irritation
- Pigmented scars on the legs often need a conservative approach
Hands
- Superficial peels may improve sun spots and uneven texture
- Skin is thinner than on the back, so treatment plans differ
Feet, elbows, knees
- Thick stratum corneum may respond to keratolytic peeling for roughness
- Scar revision results are less predictable than simple texture improvement
In practice, body peels are often most useful for:
- Back acne marks
- Chest discoloration
- Upper arm roughness with pigment
- Flat surgical scars with residual discoloration
- Mild stretch-mark texture change
Frequently Asked Questions on Chemical Peels for Body Scars
How many sessions are required for significant scar improvement?
It depends on scar depth and the type of peel.
For superficial body peels, noticeable improvement may appear after one session, especially if the target is discoloration or rough texture. More significant change usually requires a series. Clinical practice commonly uses repeated sessions spaced weeks apart. For pigment issues, some evidence from glycolic-acid literature suggests several treatments may be needed, often in the range of 6 to 8 for more visible change.
For textural scars, expectations should be modest:
- Mild PIH: often several sessions
- Shallow acne scarring: often multiple medium or repeated superficial treatments
- Deep depressed scars: peels alone may not be enough
Is it safe to perform a high-concentration TCA peel at home?
Usually, no.
This is one of the clearest answers in scar care. High-concentration TCA peels can cause burns, scarring, infection, and long-lasting dyspigmentation if used incorrectly. The risk is higher on darker skin tones and on body areas prone to friction or delayed healing. Home TCA products sold online do not change the biology of chemical injury.
Low-strength superficial formulations are very different from high-strength TCA scar techniques used in clinics. They should not be treated as interchangeable.
What are the primary risks of hyperpigmentation in darker skin tones?
The main risk is inflammation.
Any peel strong enough to create visible irritation can activate melanocytes. That may lead to:
- New dark marks around the scar
- Worsening of existing discoloration
- Uneven recovery if application is patchy or aftercare is poor
Risk increases with:
- Stronger acids
- Higher concentrations
- Repeated passes
- Sun exposure after treatment
- Picking or scrubbing peeling skin
- Preexisting eczema or active inflammation
Safer practice usually means:
- Starting with gentler acids such as lactic or mandelic
- Using test spots
- Avoiding aggressive home TCA use
- Strict sunscreen use
- Seeking clinician supervision for medium-depth peels
Conclusion
The best chemical peel for body scars is not one product or one acid. It is the treatment depth and formulation that best match the scar’s biology, the body site, and the patient’s skin tone.
Current evidence suggests:
- Superficial peels are most useful for pigmentation, roughness, and mild acne-related marks
- Medium peels may help shallow atrophic scars and more visible texture changes
- Deep peels have limited routine use for body scars because risk and downtime are substantial
- Darker skin tones require a more conservative approach because PIH risk is real
- Thick raised scars and keloids usually need treatments other than peels
For readers comparing scar options in a more structured way, the most sensible next step is a personalized review of scar type, age, symptoms, and skin tone. That can start here: Start your scar assessment.
Works Cited
- American Academy of Dermatology. "Chemical Peels: What to Know and Expect." https://www.aad.org/public/cosmetic/younger-looking/chemical-peels-overview
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.